{"title":"白内障手术后的异常炎症临床表现和发人深省的问题:这是感染还是中毒性前房综合征?","authors":"Anil Kaplan, Muhammed D Tas, Ozlem B Selver","doi":"10.4103/meajo.meajo_126_23","DOIUrl":null,"url":null,"abstract":"<p><strong>Purpose: </strong>Toxic anterior segment syndrome (TASS) is a noninfectious anterior chamber reaction caused by ocular surgeries. It usually develops within the first 12-48 h after surgery. In case of clinical suspicion of TASS, endophthalmitis as a devastating disease should always be excluded. However, the fact that TASS and endophthalmitis can look the same, but the treatment for each is different. Therefore, distinguishing between the two conditions is an important factor in coping with both diseases. It was aimed to describe the features and clinical management that are considered when distinguishing the cause of unexpected inflammatory response after cataract surgery.</p><p><strong>Methods: </strong>A retrospective review of medical records of 13 patients who developed TASS in our clinic at Ege University Ophthalmology Department on three different days between July 2022 and December 2022 were included in this study. Anterior segment photographs of those 13 patients and the records of ophthalmological examinations of those patients, including best-corrected visual acuity (BCVA), ocular pressure, biomicroscopic, and fundoscopic examination, were collected. Medical data were evaluated retrospectively.</p><p><strong>Results: </strong>The mean time to onset of clinical symptoms was 27.6 h. The main complaint was pain in nine patients. The primary symptom in the remainder of the patients was blurred vision. Severe hypopyon was seen in 5 cases. Despite the presence of pain and hypopyon, patients who were treated with topical steroids were closely followed up (every 2 h) because they were consecutive patients and had relatively acute onset complaints. Inflammation was regressed after an average of 4 h. No factor causing TASS was found. The BCVA was at the minimum level of 8/10 on the 5<sup>th</sup> day of surgery.</p><p><strong>Conclusion: </strong>When distinguishing TASS from endophthalmitis, severe pain, relatively late onset, hyperemia, and the presence of severe hypopyon usually lead ophthalmologists to the clinical diagnosis of endophthalmitis. However, in this study, most of the patients diagnosed with TASS had severe pain, a significant portion of them had hypopyon, and the onset of the symptoms was relatively late. Close follow-up immediately after suspicion plays a vital role in clinical diagnosis and management accordingly.</p>","PeriodicalId":18740,"journal":{"name":"Middle East African Journal of Ophthalmology","volume":"29 4","pages":"196-199"},"PeriodicalIF":0.3000,"publicationDate":"2023-11-21","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10754112/pdf/","citationCount":"0","resultStr":"{\"title\":\"Unusual Inflammatory Clinical Presentation After Cataract Surgery and that Thought-provoking Question: Is this Infection or Toxic Anterior Segment Syndrome?\",\"authors\":\"Anil Kaplan, Muhammed D Tas, Ozlem B Selver\",\"doi\":\"10.4103/meajo.meajo_126_23\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Purpose: </strong>Toxic anterior segment syndrome (TASS) is a noninfectious anterior chamber reaction caused by ocular surgeries. It usually develops within the first 12-48 h after surgery. In case of clinical suspicion of TASS, endophthalmitis as a devastating disease should always be excluded. However, the fact that TASS and endophthalmitis can look the same, but the treatment for each is different. Therefore, distinguishing between the two conditions is an important factor in coping with both diseases. It was aimed to describe the features and clinical management that are considered when distinguishing the cause of unexpected inflammatory response after cataract surgery.</p><p><strong>Methods: </strong>A retrospective review of medical records of 13 patients who developed TASS in our clinic at Ege University Ophthalmology Department on three different days between July 2022 and December 2022 were included in this study. Anterior segment photographs of those 13 patients and the records of ophthalmological examinations of those patients, including best-corrected visual acuity (BCVA), ocular pressure, biomicroscopic, and fundoscopic examination, were collected. Medical data were evaluated retrospectively.</p><p><strong>Results: </strong>The mean time to onset of clinical symptoms was 27.6 h. The main complaint was pain in nine patients. The primary symptom in the remainder of the patients was blurred vision. Severe hypopyon was seen in 5 cases. Despite the presence of pain and hypopyon, patients who were treated with topical steroids were closely followed up (every 2 h) because they were consecutive patients and had relatively acute onset complaints. Inflammation was regressed after an average of 4 h. No factor causing TASS was found. The BCVA was at the minimum level of 8/10 on the 5<sup>th</sup> day of surgery.</p><p><strong>Conclusion: </strong>When distinguishing TASS from endophthalmitis, severe pain, relatively late onset, hyperemia, and the presence of severe hypopyon usually lead ophthalmologists to the clinical diagnosis of endophthalmitis. However, in this study, most of the patients diagnosed with TASS had severe pain, a significant portion of them had hypopyon, and the onset of the symptoms was relatively late. Close follow-up immediately after suspicion plays a vital role in clinical diagnosis and management accordingly.</p>\",\"PeriodicalId\":18740,\"journal\":{\"name\":\"Middle East African Journal of Ophthalmology\",\"volume\":\"29 4\",\"pages\":\"196-199\"},\"PeriodicalIF\":0.3000,\"publicationDate\":\"2023-11-21\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10754112/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Middle East African Journal of Ophthalmology\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.4103/meajo.meajo_126_23\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2022/10/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q4\",\"JCRName\":\"OPHTHALMOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Middle East African Journal of Ophthalmology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.4103/meajo.meajo_126_23","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2022/10/1 0:00:00","PubModel":"eCollection","JCR":"Q4","JCRName":"OPHTHALMOLOGY","Score":null,"Total":0}
Unusual Inflammatory Clinical Presentation After Cataract Surgery and that Thought-provoking Question: Is this Infection or Toxic Anterior Segment Syndrome?
Purpose: Toxic anterior segment syndrome (TASS) is a noninfectious anterior chamber reaction caused by ocular surgeries. It usually develops within the first 12-48 h after surgery. In case of clinical suspicion of TASS, endophthalmitis as a devastating disease should always be excluded. However, the fact that TASS and endophthalmitis can look the same, but the treatment for each is different. Therefore, distinguishing between the two conditions is an important factor in coping with both diseases. It was aimed to describe the features and clinical management that are considered when distinguishing the cause of unexpected inflammatory response after cataract surgery.
Methods: A retrospective review of medical records of 13 patients who developed TASS in our clinic at Ege University Ophthalmology Department on three different days between July 2022 and December 2022 were included in this study. Anterior segment photographs of those 13 patients and the records of ophthalmological examinations of those patients, including best-corrected visual acuity (BCVA), ocular pressure, biomicroscopic, and fundoscopic examination, were collected. Medical data were evaluated retrospectively.
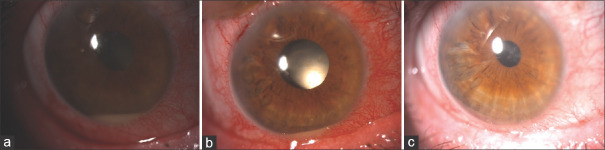
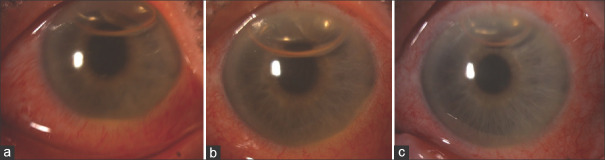
Results: The mean time to onset of clinical symptoms was 27.6 h. The main complaint was pain in nine patients. The primary symptom in the remainder of the patients was blurred vision. Severe hypopyon was seen in 5 cases. Despite the presence of pain and hypopyon, patients who were treated with topical steroids were closely followed up (every 2 h) because they were consecutive patients and had relatively acute onset complaints. Inflammation was regressed after an average of 4 h. No factor causing TASS was found. The BCVA was at the minimum level of 8/10 on the 5th day of surgery.
Conclusion: When distinguishing TASS from endophthalmitis, severe pain, relatively late onset, hyperemia, and the presence of severe hypopyon usually lead ophthalmologists to the clinical diagnosis of endophthalmitis. However, in this study, most of the patients diagnosed with TASS had severe pain, a significant portion of them had hypopyon, and the onset of the symptoms was relatively late. Close follow-up immediately after suspicion plays a vital role in clinical diagnosis and management accordingly.
期刊介绍:
The Middle East African Journal of Ophthalmology (MEAJO), published four times per year in print and online, is an official journal of the Middle East African Council of Ophthalmology (MEACO). It is an international, peer-reviewed journal whose mission includes publication of original research of interest to ophthalmologists in the Middle East and Africa, and to provide readers with high quality educational review articles from world-renown experts. MEAJO, previously known as Middle East Journal of Ophthalmology (MEJO) was founded by Dr Akef El Maghraby in 1993.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
