Alex F. Peahl MD, MSc, Lisa Kane Low PhD, MS, CNM, Elizabeth S. Langen MD, Michelle H. Moniz MD, MSc, Bryan Aaron BS, Hsou Mei Hu PhD, MBA, MHS, Jennifer Waljee MD, MPH, Courtney Townsel MD, MSc
{"title":"参与全州产科护理质量合作的医院产后阿片类药物处方差异的驱动因素。","authors":"Alex F. Peahl MD, MSc, Lisa Kane Low PhD, MS, CNM, Elizabeth S. Langen MD, Michelle H. Moniz MD, MSc, Bryan Aaron BS, Hsou Mei Hu PhD, MBA, MHS, Jennifer Waljee MD, MPH, Courtney Townsel MD, MSc","doi":"10.1111/birt.12809","DOIUrl":null,"url":null,"abstract":"<div>\n \n \n <section>\n \n <h3> Background</h3>\n \n <p>We describe variation in postpartum opioid prescribing across a statewide quality collaborative and assess the proportion due to practitioner and hospital characteristics.</p>\n </section>\n \n <section>\n \n <h3> Methods</h3>\n \n <p>We assessed postpartum prescribing data from nulliparous, term, singleton, vertex births between January 2020 and June 2021 included in the clinical registry of a statewide obstetric quality collaborative funded by Blue Cross Blue Shield of Michigan. Data were summarized using descriptive statistics. Mixed effect logistic regression and linear models adjusted for patient characteristics and assessed practitioner- and hospital-level predictors of receiving a postpartum opioid prescription and prescription size. Relative contributions of practitioner and hospital characteristics were assessed using the intraclass correlation coefficient.</p>\n </section>\n \n <section>\n \n <h3> Results</h3>\n \n <p>Of 40,589 patients birthing at 68 hospitals, 3.0% (872/29,412) received an opioid prescription after vaginal birth and 87.8% (9812/11,177) received one after cesarean birth, with high variation across hospitals. In adjusted models, the strongest patient-level predictors of receiving a prescription were cesarean birth (aOR 899.1, 95% CI 752.8–1066.7) and third−/fourth-degree perineal laceration (aOR 25.7, 95% CI 17.4–37.9). Receiving care from a certified nurse-midwife (aOR 0.63, 95% CI 0.48–0.82) or family medicine physician (aOR 0.60, 95%CI 0.39–0.91) was associated with lower prescribing rates. Hospital-level predictors included receiving care at hospitals with <500 annual births (aOR 4.07, 95% CI 1.61–15.0). A positive safety culture was associated with lower prescribing rates (aOR 0.37, 95% CI 0.15–0.88). Much of the variation in postpartum prescribing was attributable to practitioners and hospitals (prescription receipt: practitioners 25.1%, hospitals 12.1%; prescription size: practitioners 5.4%, hospitals: 52.2%).</p>\n </section>\n \n <section>\n \n <h3> Discussion</h3>\n \n <p>Variation in postpartum opioid prescribing after birth is high and driven largely by practitioner- and hospital-level factors. Opioid stewardship efforts targeted at both the practitioner and hospital level may be effective for reducing opioid prescribing harms.</p>\n </section>\n </div>","PeriodicalId":55350,"journal":{"name":"Birth-Issues in Perinatal Care","volume":"51 3","pages":"541-558"},"PeriodicalIF":2.5000,"publicationDate":"2023-12-30","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11214638/pdf/","citationCount":"0","resultStr":"{\"title\":\"Drivers of variation in postpartum opioid prescribing across hospitals participating in a statewide maternity care quality collaborative\",\"authors\":\"Alex F. Peahl MD, MSc, Lisa Kane Low PhD, MS, CNM, Elizabeth S. Langen MD, Michelle H. Moniz MD, MSc, Bryan Aaron BS, Hsou Mei Hu PhD, MBA, MHS, Jennifer Waljee MD, MPH, Courtney Townsel MD, MSc\",\"doi\":\"10.1111/birt.12809\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<div>\\n \\n \\n <section>\\n \\n <h3> Background</h3>\\n \\n <p>We describe variation in postpartum opioid prescribing across a statewide quality collaborative and assess the proportion due to practitioner and hospital characteristics.</p>\\n </section>\\n \\n <section>\\n \\n <h3> Methods</h3>\\n \\n <p>We assessed postpartum prescribing data from nulliparous, term, singleton, vertex births between January 2020 and June 2021 included in the clinical registry of a statewide obstetric quality collaborative funded by Blue Cross Blue Shield of Michigan. Data were summarized using descriptive statistics. Mixed effect logistic regression and linear models adjusted for patient characteristics and assessed practitioner- and hospital-level predictors of receiving a postpartum opioid prescription and prescription size. Relative contributions of practitioner and hospital characteristics were assessed using the intraclass correlation coefficient.</p>\\n </section>\\n \\n <section>\\n \\n <h3> Results</h3>\\n \\n <p>Of 40,589 patients birthing at 68 hospitals, 3.0% (872/29,412) received an opioid prescription after vaginal birth and 87.8% (9812/11,177) received one after cesarean birth, with high variation across hospitals. In adjusted models, the strongest patient-level predictors of receiving a prescription were cesarean birth (aOR 899.1, 95% CI 752.8–1066.7) and third−/fourth-degree perineal laceration (aOR 25.7, 95% CI 17.4–37.9). Receiving care from a certified nurse-midwife (aOR 0.63, 95% CI 0.48–0.82) or family medicine physician (aOR 0.60, 95%CI 0.39–0.91) was associated with lower prescribing rates. Hospital-level predictors included receiving care at hospitals with <500 annual births (aOR 4.07, 95% CI 1.61–15.0). A positive safety culture was associated with lower prescribing rates (aOR 0.37, 95% CI 0.15–0.88). Much of the variation in postpartum prescribing was attributable to practitioners and hospitals (prescription receipt: practitioners 25.1%, hospitals 12.1%; prescription size: practitioners 5.4%, hospitals: 52.2%).</p>\\n </section>\\n \\n <section>\\n \\n <h3> Discussion</h3>\\n \\n <p>Variation in postpartum opioid prescribing after birth is high and driven largely by practitioner- and hospital-level factors. Opioid stewardship efforts targeted at both the practitioner and hospital level may be effective for reducing opioid prescribing harms.</p>\\n </section>\\n </div>\",\"PeriodicalId\":55350,\"journal\":{\"name\":\"Birth-Issues in Perinatal Care\",\"volume\":\"51 3\",\"pages\":\"541-558\"},\"PeriodicalIF\":2.5000,\"publicationDate\":\"2023-12-30\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11214638/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Birth-Issues in Perinatal Care\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://onlinelibrary.wiley.com/doi/10.1111/birt.12809\",\"RegionNum\":3,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q1\",\"JCRName\":\"NURSING\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Birth-Issues in Perinatal Care","FirstCategoryId":"3","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1111/birt.12809","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"NURSING","Score":null,"Total":0}
引用次数: 0
摘要
背景:我们描述了全州质量合作组织产后阿片类药物处方的差异,并评估了因从业人员和医院特征造成的比例:我们评估了 2020 年 1 月至 2021 年 6 月期间由密歇根州蓝十字蓝盾公司资助的全州产科质量合作临床登记册中的无胎儿、足月、单胎、顶点分娩的产后处方数据。数据采用描述性统计进行汇总。混合效应逻辑回归和线性模型对患者特征进行了调整,并评估了从业人员和医院层面对产后接受阿片类药物处方和处方量的预测因素。使用类内相关系数评估了从业人员和医院特征的相对贡献:在 68 家医院分娩的 40,589 名患者中,3.0%(872/29,412)的患者在阴道分娩后获得了阿片类药物处方,87.8%(9812/11,177)的患者在剖宫产后获得了阿片类药物处方,不同医院之间的差异很大。在调整后的模型中,剖宫产(aOR 899.1,95% CI 752.8-1066.7)和三度/四度会阴裂伤(aOR 25.7,95% CI 17.4-37.9)是患者获得处方的最强预测因素。接受注册助产士(aOR 0.63,95% CI 0.48-0.82)或家庭医生(aOR 0.60,95%CI 0.39-0.91)护理与较低的处方率有关。医院层面的预测因素包括在有讨论的医院接受治疗:产后阿片类药物处方的变化很大,主要受执业医师和医院层面因素的影响。针对执业医师和医院层面的阿片类药物管理措施可能会有效减少阿片类药物处方的危害。
Drivers of variation in postpartum opioid prescribing across hospitals participating in a statewide maternity care quality collaborative
Background
We describe variation in postpartum opioid prescribing across a statewide quality collaborative and assess the proportion due to practitioner and hospital characteristics.
Methods
We assessed postpartum prescribing data from nulliparous, term, singleton, vertex births between January 2020 and June 2021 included in the clinical registry of a statewide obstetric quality collaborative funded by Blue Cross Blue Shield of Michigan. Data were summarized using descriptive statistics. Mixed effect logistic regression and linear models adjusted for patient characteristics and assessed practitioner- and hospital-level predictors of receiving a postpartum opioid prescription and prescription size. Relative contributions of practitioner and hospital characteristics were assessed using the intraclass correlation coefficient.
Results
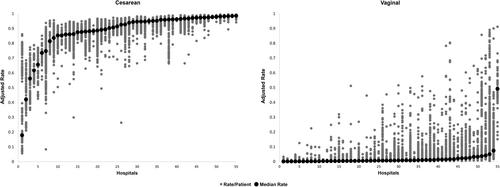
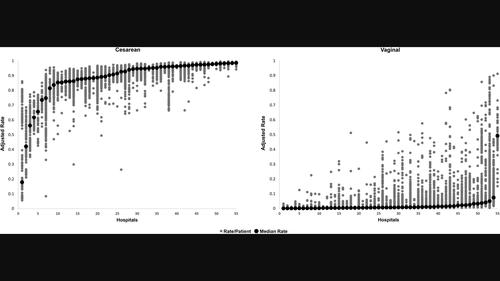
Of 40,589 patients birthing at 68 hospitals, 3.0% (872/29,412) received an opioid prescription after vaginal birth and 87.8% (9812/11,177) received one after cesarean birth, with high variation across hospitals. In adjusted models, the strongest patient-level predictors of receiving a prescription were cesarean birth (aOR 899.1, 95% CI 752.8–1066.7) and third−/fourth-degree perineal laceration (aOR 25.7, 95% CI 17.4–37.9). Receiving care from a certified nurse-midwife (aOR 0.63, 95% CI 0.48–0.82) or family medicine physician (aOR 0.60, 95%CI 0.39–0.91) was associated with lower prescribing rates. Hospital-level predictors included receiving care at hospitals with <500 annual births (aOR 4.07, 95% CI 1.61–15.0). A positive safety culture was associated with lower prescribing rates (aOR 0.37, 95% CI 0.15–0.88). Much of the variation in postpartum prescribing was attributable to practitioners and hospitals (prescription receipt: practitioners 25.1%, hospitals 12.1%; prescription size: practitioners 5.4%, hospitals: 52.2%).
Discussion
Variation in postpartum opioid prescribing after birth is high and driven largely by practitioner- and hospital-level factors. Opioid stewardship efforts targeted at both the practitioner and hospital level may be effective for reducing opioid prescribing harms.
期刊介绍:
Birth: Issues in Perinatal Care is a multidisciplinary, refereed journal devoted to issues and practices in the care of childbearing women, infants, and families. It is written by and for professionals in maternal and neonatal health, nurses, midwives, physicians, public health workers, doulas, social scientists, childbirth educators, lactation counselors, epidemiologists, and other health caregivers and policymakers in perinatal care.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
