Dong Hee Jang, Dong-Hee Kim, Eun Seok Choi, Tae-Jin Yun, Chun Soo Park
{"title":"在婴儿期使用右心室和肺动脉之间的导管进行双心室修复后的效果。","authors":"Dong Hee Jang, Dong-Hee Kim, Eun Seok Choi, Tae-Jin Yun, Chun Soo Park","doi":"10.5090/jcs.23.107","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>This study investigated the outcomes of biventricular repair using right ventricle to pulmonary artery (RV-PA) conduit placement in patients aged <1 year.</p><p><strong>Methods: </strong>Patients aged <1 year who underwent biventricular repair using an RV-PA conduit between 2011 and 2020 were included in this study. The outcomes of interest were death from any cause, conduit reintervention, and conduit dysfunction (peak velocity of ≥3.5 m/sec or moderate or severe regurgitation).</p><p><strong>Results: </strong>In total, 141 patients were enrolled. The median age at initial conduit implantation was 6 months. The median conduit diameter z-score was 1.3. The overall 5-year survival rate was 89.6%. In the multivariable analysis, younger age (p=0.006) and longer cardiopulmonary bypass time (p=0.001) were risk factors for overall mortality. During follow-up, 61 patients required conduit reintervention, and conduit dysfunction occurred in 68 patients. The 5-year freedom from conduit reintervention and dysfunction rates were 52.9% and 45.9%, respectively. In the multivariable analysis, a smaller conduit z-score (p<0.001) was a shared risk factor for both conduit reintervention and dysfunction. Analysis of variance demonstrated a nonlinear relationship between the conduit z-score and conduit reintervention or dysfunction. The hazard ratio was lowest in patients with a conduit z-score of 1.3 for reintervention and a conduit z-score of 1.4 for dysfunction.</p><p><strong>Conclusion: </strong>RV-PA conduit placement can be safely performed in infants. A significant number of patients required conduit reintervention and had conduit dysfunction. A slightly oversized conduit with a z-score of 1.3 may reduce the risk of conduit reintervention or dysfunction.</p>","PeriodicalId":34499,"journal":{"name":"Journal of Chest Surgery","volume":"57 1","pages":"70-78"},"PeriodicalIF":1.0000,"publicationDate":"2024-01-05","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10792375/pdf/","citationCount":"0","resultStr":"{\"title\":\"Outcomes after Biventricular Repair Using a Conduit between the Right Ventricle and Pulmonary Artery in Infancy.\",\"authors\":\"Dong Hee Jang, Dong-Hee Kim, Eun Seok Choi, Tae-Jin Yun, Chun Soo Park\",\"doi\":\"10.5090/jcs.23.107\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>This study investigated the outcomes of biventricular repair using right ventricle to pulmonary artery (RV-PA) conduit placement in patients aged <1 year.</p><p><strong>Methods: </strong>Patients aged <1 year who underwent biventricular repair using an RV-PA conduit between 2011 and 2020 were included in this study. The outcomes of interest were death from any cause, conduit reintervention, and conduit dysfunction (peak velocity of ≥3.5 m/sec or moderate or severe regurgitation).</p><p><strong>Results: </strong>In total, 141 patients were enrolled. The median age at initial conduit implantation was 6 months. The median conduit diameter z-score was 1.3. The overall 5-year survival rate was 89.6%. In the multivariable analysis, younger age (p=0.006) and longer cardiopulmonary bypass time (p=0.001) were risk factors for overall mortality. During follow-up, 61 patients required conduit reintervention, and conduit dysfunction occurred in 68 patients. The 5-year freedom from conduit reintervention and dysfunction rates were 52.9% and 45.9%, respectively. In the multivariable analysis, a smaller conduit z-score (p<0.001) was a shared risk factor for both conduit reintervention and dysfunction. Analysis of variance demonstrated a nonlinear relationship between the conduit z-score and conduit reintervention or dysfunction. The hazard ratio was lowest in patients with a conduit z-score of 1.3 for reintervention and a conduit z-score of 1.4 for dysfunction.</p><p><strong>Conclusion: </strong>RV-PA conduit placement can be safely performed in infants. A significant number of patients required conduit reintervention and had conduit dysfunction. A slightly oversized conduit with a z-score of 1.3 may reduce the risk of conduit reintervention or dysfunction.</p>\",\"PeriodicalId\":34499,\"journal\":{\"name\":\"Journal of Chest Surgery\",\"volume\":\"57 1\",\"pages\":\"70-78\"},\"PeriodicalIF\":1.0000,\"publicationDate\":\"2024-01-05\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10792375/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of Chest Surgery\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.5090/jcs.23.107\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q4\",\"JCRName\":\"Medicine\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Chest Surgery","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.5090/jcs.23.107","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q4","JCRName":"Medicine","Score":null,"Total":0}
Outcomes after Biventricular Repair Using a Conduit between the Right Ventricle and Pulmonary Artery in Infancy.
Background: This study investigated the outcomes of biventricular repair using right ventricle to pulmonary artery (RV-PA) conduit placement in patients aged <1 year.
Methods: Patients aged <1 year who underwent biventricular repair using an RV-PA conduit between 2011 and 2020 were included in this study. The outcomes of interest were death from any cause, conduit reintervention, and conduit dysfunction (peak velocity of ≥3.5 m/sec or moderate or severe regurgitation).
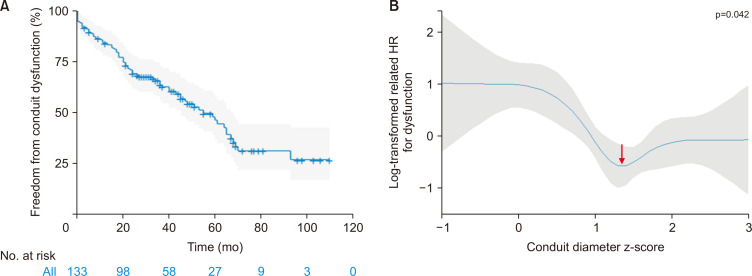
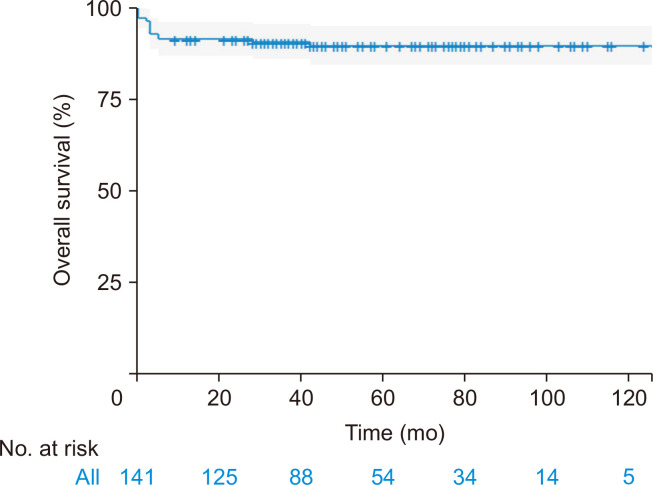
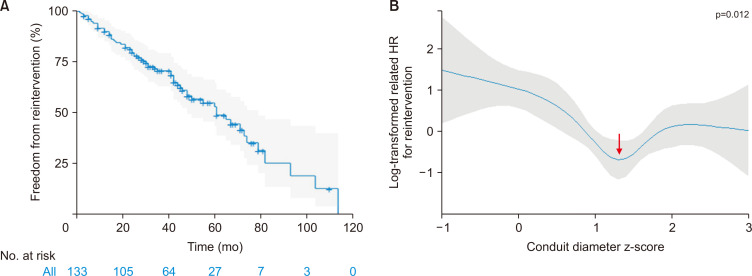
Results: In total, 141 patients were enrolled. The median age at initial conduit implantation was 6 months. The median conduit diameter z-score was 1.3. The overall 5-year survival rate was 89.6%. In the multivariable analysis, younger age (p=0.006) and longer cardiopulmonary bypass time (p=0.001) were risk factors for overall mortality. During follow-up, 61 patients required conduit reintervention, and conduit dysfunction occurred in 68 patients. The 5-year freedom from conduit reintervention and dysfunction rates were 52.9% and 45.9%, respectively. In the multivariable analysis, a smaller conduit z-score (p<0.001) was a shared risk factor for both conduit reintervention and dysfunction. Analysis of variance demonstrated a nonlinear relationship between the conduit z-score and conduit reintervention or dysfunction. The hazard ratio was lowest in patients with a conduit z-score of 1.3 for reintervention and a conduit z-score of 1.4 for dysfunction.
Conclusion: RV-PA conduit placement can be safely performed in infants. A significant number of patients required conduit reintervention and had conduit dysfunction. A slightly oversized conduit with a z-score of 1.3 may reduce the risk of conduit reintervention or dysfunction.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
