Jason J Sico, Xin Hu, Laura J Myers, Deborah Levine, Dawn M Bravata, Greg W Arling
{"title":"两种缺血性中风和 TIA 收缩压目标对 12 个月死亡率和复发性血管事件的真实世界分析。","authors":"Jason J Sico, Xin Hu, Laura J Myers, Deborah Levine, Dawn M Bravata, Greg W Arling","doi":"10.1136/svn-2023-002759","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>Whether obtaining the more intensive goal systolic blood pressure (SBP) of <130 mm Hg, rather than a less intensive SBP goal of <140 mm Hg poststroke/transient ischaemic attack (TIA) is associated with incremental mortality and recurrent vascular event benefit is largely unexplored using real-world data. Lowering SBP excessively may result in poorer outcomes.</p><p><strong>Methods: </strong>This is a retrospective cohort study of 26 368 Veterans presenting to a Veterans Administration Medical Center (VAMC) with a stroke/TIA between October 2015 and July 2018. Patients were excluded from the study if they had missing or extreme BP values, receiving dialysis or palliative care, left against medical advice had a cancer diagnosis, were cared for in a VAMC enrolled in a stroke/TIA quality improvement initiative, died or had a cerebrovascular or cardiovascular event within 90 days after their index stroke/TIA. The analytical sample included 12 337 patients. Average SBP during 90 days after discharge was assessed in categories (≤105 mm Hg, 106-115 mm Hg, 116-130 mm Hg, 131-140 mm Hg and >140 mm Hg). Separate multivariable Cox proportional hazard regressions were used to examine the relationship between average SBP groups and time to: (1) mortality and (2) any recurrent vascular event, from 90 days to up to 365 days after discharge from the index emergency department visit or inpatient admission.</p><p><strong>Results: </strong>Compared with those with SBP>140 mm Hg, patients with SBP between 116 and 130 mm Hg had a significantly lower risk of recurrent stroke/TIA (HR 0.77, 95% CI 0.60 to 0.99) but not cardiovascular events. Patients with SBP lower than 105 mm Hg, compared with those with >140 mm Hg demonstrated a statistically significant higher risk of death (HR 2.07, 95% CI 1.43 to 3.00), but no statistical differences were found in other SBP groups.</p><p><strong>Discussion: </strong>Data support a more intensive SBP goal to prevent recurrent cerebrovascular events among stroke/TIA patients by 90 days poststroke/TIA compared with less intensive goal. Very low SBPs were associated with increased mortality risk.</p>","PeriodicalId":48733,"journal":{"name":"Journal of Investigative Medicine","volume":" ","pages":"519-529"},"PeriodicalIF":4.9000,"publicationDate":"2024-11-05","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11732840/pdf/","citationCount":"0","resultStr":"{\"title\":\"Real-world analysis of two ischaemic stroke and TIA systolic blood pressure goals on 12-month mortality and recurrent vascular events.\",\"authors\":\"Jason J Sico, Xin Hu, Laura J Myers, Deborah Levine, Dawn M Bravata, Greg W Arling\",\"doi\":\"10.1136/svn-2023-002759\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Introduction: </strong>Whether obtaining the more intensive goal systolic blood pressure (SBP) of <130 mm Hg, rather than a less intensive SBP goal of <140 mm Hg poststroke/transient ischaemic attack (TIA) is associated with incremental mortality and recurrent vascular event benefit is largely unexplored using real-world data. Lowering SBP excessively may result in poorer outcomes.</p><p><strong>Methods: </strong>This is a retrospective cohort study of 26 368 Veterans presenting to a Veterans Administration Medical Center (VAMC) with a stroke/TIA between October 2015 and July 2018. Patients were excluded from the study if they had missing or extreme BP values, receiving dialysis or palliative care, left against medical advice had a cancer diagnosis, were cared for in a VAMC enrolled in a stroke/TIA quality improvement initiative, died or had a cerebrovascular or cardiovascular event within 90 days after their index stroke/TIA. The analytical sample included 12 337 patients. Average SBP during 90 days after discharge was assessed in categories (≤105 mm Hg, 106-115 mm Hg, 116-130 mm Hg, 131-140 mm Hg and >140 mm Hg). Separate multivariable Cox proportional hazard regressions were used to examine the relationship between average SBP groups and time to: (1) mortality and (2) any recurrent vascular event, from 90 days to up to 365 days after discharge from the index emergency department visit or inpatient admission.</p><p><strong>Results: </strong>Compared with those with SBP>140 mm Hg, patients with SBP between 116 and 130 mm Hg had a significantly lower risk of recurrent stroke/TIA (HR 0.77, 95% CI 0.60 to 0.99) but not cardiovascular events. Patients with SBP lower than 105 mm Hg, compared with those with >140 mm Hg demonstrated a statistically significant higher risk of death (HR 2.07, 95% CI 1.43 to 3.00), but no statistical differences were found in other SBP groups.</p><p><strong>Discussion: </strong>Data support a more intensive SBP goal to prevent recurrent cerebrovascular events among stroke/TIA patients by 90 days poststroke/TIA compared with less intensive goal. Very low SBPs were associated with increased mortality risk.</p>\",\"PeriodicalId\":48733,\"journal\":{\"name\":\"Journal of Investigative Medicine\",\"volume\":\" \",\"pages\":\"519-529\"},\"PeriodicalIF\":4.9000,\"publicationDate\":\"2024-11-05\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11732840/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of Investigative Medicine\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1136/svn-2023-002759\",\"RegionNum\":1,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Investigative Medicine","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1136/svn-2023-002759","RegionNum":1,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
摘要
介绍:是否能获得更高强度的收缩压(SBP)目标方法:这是一项回顾性队列研究,研究对象是 2015 年 10 月至 2018 年 7 月期间因中风/TIA 到退伍军人管理医疗中心(VAMC)就诊的 26 368 名退伍军人。如果患者血压值缺失或极值、接受透析或姑息治疗、违背医嘱离开、确诊癌症、在参与卒中/TIA 质量改进计划的退伍军人管理医疗中心接受治疗、死亡或在卒中/TIA 发生后 90 天内发生脑血管或心血管事件,则将其排除在研究之外。分析样本包括 12 337 名患者。对出院后 90 天内的平均 SBP 进行了分类评估(≤105 mm Hg、106-115 mm Hg、116-130 mm Hg、131-140 mm Hg 和 >140 mm Hg)。分别采用多变量考克斯比例危险回归法来检验平均 SBP 组别与以下时间之间的关系:(1) 死亡率;(2) 平均 SBP 组别与以下时间之间的关系:结果发现,在急诊科就诊或住院患者出院后 90 天至 365 天内,平均 SBP 组别与以下事件发生时间之间的关系为:(1) 死亡率;(2) 任何复发性血管事件:与 SBP>140 mm Hg 的患者相比,SBP 在 116-130 mm Hg 之间的患者发生复发性卒中/TIA 的风险明显降低(HR 0.77,95% CI 0.60-0.99),但心血管事件的风险却没有降低。SBP低于105毫米汞柱的患者与SBP高于140毫米汞柱的患者相比,死亡风险明显更高(HR为2.07,95% CI为1.43至3.00),但其他SBP组没有发现统计学差异:讨论:与强度较低的目标相比,数据支持为预防卒中/TIA 患者在卒中/TIA 后 90 天内再次发生脑血管事件而制定强度更高的 SBP 目标。极低的 SBP 与死亡风险增加有关。
Real-world analysis of two ischaemic stroke and TIA systolic blood pressure goals on 12-month mortality and recurrent vascular events.
Introduction: Whether obtaining the more intensive goal systolic blood pressure (SBP) of <130 mm Hg, rather than a less intensive SBP goal of <140 mm Hg poststroke/transient ischaemic attack (TIA) is associated with incremental mortality and recurrent vascular event benefit is largely unexplored using real-world data. Lowering SBP excessively may result in poorer outcomes.
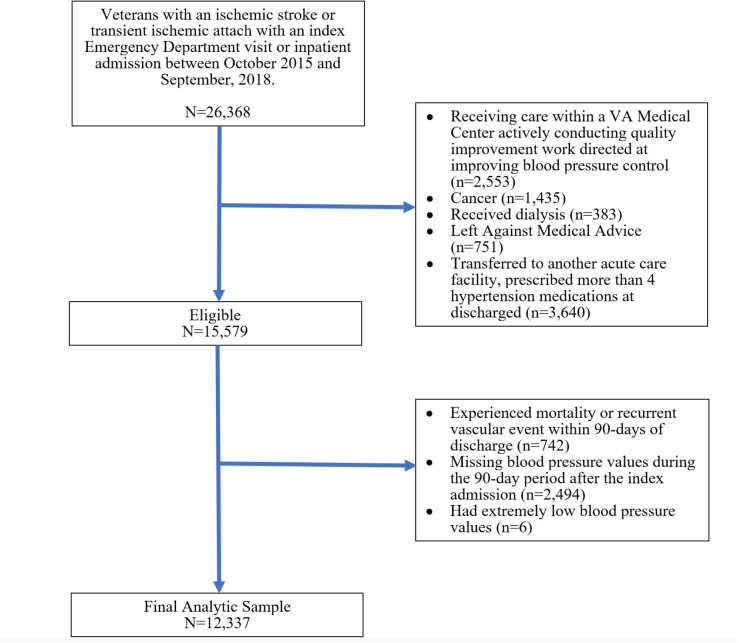
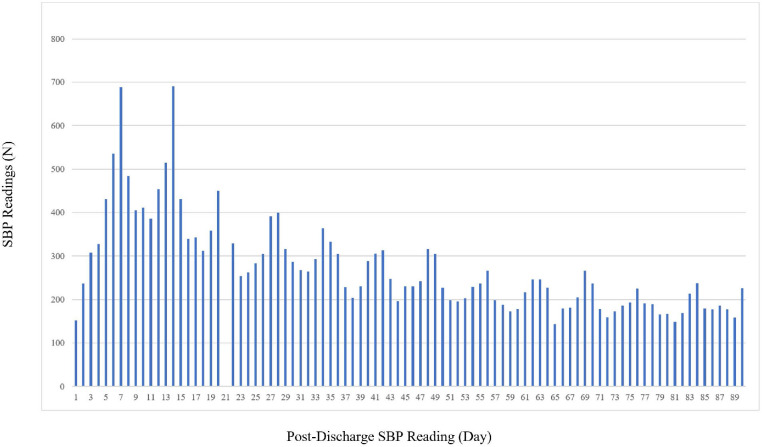
Methods: This is a retrospective cohort study of 26 368 Veterans presenting to a Veterans Administration Medical Center (VAMC) with a stroke/TIA between October 2015 and July 2018. Patients were excluded from the study if they had missing or extreme BP values, receiving dialysis or palliative care, left against medical advice had a cancer diagnosis, were cared for in a VAMC enrolled in a stroke/TIA quality improvement initiative, died or had a cerebrovascular or cardiovascular event within 90 days after their index stroke/TIA. The analytical sample included 12 337 patients. Average SBP during 90 days after discharge was assessed in categories (≤105 mm Hg, 106-115 mm Hg, 116-130 mm Hg, 131-140 mm Hg and >140 mm Hg). Separate multivariable Cox proportional hazard regressions were used to examine the relationship between average SBP groups and time to: (1) mortality and (2) any recurrent vascular event, from 90 days to up to 365 days after discharge from the index emergency department visit or inpatient admission.
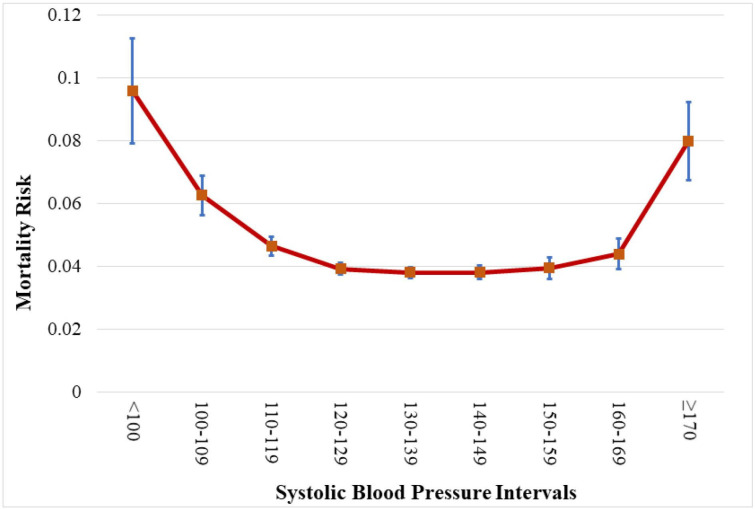
Results: Compared with those with SBP>140 mm Hg, patients with SBP between 116 and 130 mm Hg had a significantly lower risk of recurrent stroke/TIA (HR 0.77, 95% CI 0.60 to 0.99) but not cardiovascular events. Patients with SBP lower than 105 mm Hg, compared with those with >140 mm Hg demonstrated a statistically significant higher risk of death (HR 2.07, 95% CI 1.43 to 3.00), but no statistical differences were found in other SBP groups.
Discussion: Data support a more intensive SBP goal to prevent recurrent cerebrovascular events among stroke/TIA patients by 90 days poststroke/TIA compared with less intensive goal. Very low SBPs were associated with increased mortality risk.
期刊介绍:
Journal of Investigative Medicine (JIM) is the official publication of the American Federation for Medical Research. The journal is peer-reviewed and publishes high-quality original articles and reviews in the areas of basic, clinical, and translational medical research.
JIM publishes on all topics and specialty areas that are critical to the conduct of the entire spectrum of biomedical research: from the translation of clinical observations at the bedside, to basic and animal research to clinical research and the implementation of innovative medical care.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
