Pietro Quaretti, Riccardo Corti, Antonio Mauro D'Agostino, Antonio Bozzani, Lorenzo Paolo Moramarco, Nicola Cionfoli
{"title":"覆盖支架辅助线圈栓塞慢性腹腔干闭塞的大型布勒动脉瘤。","authors":"Pietro Quaretti, Riccardo Corti, Antonio Mauro D'Agostino, Antonio Bozzani, Lorenzo Paolo Moramarco, Nicola Cionfoli","doi":"10.1186/s42155-023-00416-4","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>The arc of Bühler (AOB) is a residual embryonal anastomosis between the celiac artery (CA) and the superior mesenteric artery (SMA). Although usually asymptomatic, it has clinical relevance when compensatory reverse flow between the SMA and the CA in response to celiac artery obstruction leads to aneurysm formation and bleeding. Endovascular coiling is the mainstay therapy because of the deep AOB retropancreatic location, which hinders open surgery.</p><p><strong>Case presentation: </strong>We herein report a case of a 2.8-cm AOB saccular aneurysm and LAM compression of celiac trunk in a 47-year-old man during rehabilitation following motorcycle trauma and vertebral surgery. The patient was considered unsuitable for surgery. Neither conventional coiling nor bare-metal stent and balloon-assisted techniques for coiling were suitable because of the wide necked saccular shape of AOB aneurysm interposed between the SMA and the floor of celiac trunk. To exclude the aneurysm from direct SMA inflow and permit safe and efficient coiling to rule out retrograde sac perfusion, a 9-mm polytetrafluoroethylene stent graft (Viabahn; Gore, Phoenix, AZ, USA) was positioned in the mesenteric artery, followed by antegrade periprosthetic high-density packed coiling of the aneurysm. The AOB remained excluded from mesenteric perfusion. The patient's clinical condition and abdominal contrast-enhanced multislice computed tomographic findings were unremarkable at the 9-year follow-up.</p><p><strong>Conclusion: </strong>The 9 year long-term efficacy in our case raises the possibility that perigraft coiling following stent-graft deployment in the SMA may represent a valuable technical option for large Bühler aneurysms that are not amenable to stand-alone coiling.</p>","PeriodicalId":52351,"journal":{"name":"CVIR Endovascular","volume":"7 1","pages":"9"},"PeriodicalIF":2.1000,"publicationDate":"2024-01-10","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10781915/pdf/","citationCount":"0","resultStr":"{\"title\":\"Covered stent assisted coil embolization of large Buhler aneurysm in setting of chronic celiac trunk occlusion.\",\"authors\":\"Pietro Quaretti, Riccardo Corti, Antonio Mauro D'Agostino, Antonio Bozzani, Lorenzo Paolo Moramarco, Nicola Cionfoli\",\"doi\":\"10.1186/s42155-023-00416-4\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>The arc of Bühler (AOB) is a residual embryonal anastomosis between the celiac artery (CA) and the superior mesenteric artery (SMA). Although usually asymptomatic, it has clinical relevance when compensatory reverse flow between the SMA and the CA in response to celiac artery obstruction leads to aneurysm formation and bleeding. Endovascular coiling is the mainstay therapy because of the deep AOB retropancreatic location, which hinders open surgery.</p><p><strong>Case presentation: </strong>We herein report a case of a 2.8-cm AOB saccular aneurysm and LAM compression of celiac trunk in a 47-year-old man during rehabilitation following motorcycle trauma and vertebral surgery. The patient was considered unsuitable for surgery. Neither conventional coiling nor bare-metal stent and balloon-assisted techniques for coiling were suitable because of the wide necked saccular shape of AOB aneurysm interposed between the SMA and the floor of celiac trunk. To exclude the aneurysm from direct SMA inflow and permit safe and efficient coiling to rule out retrograde sac perfusion, a 9-mm polytetrafluoroethylene stent graft (Viabahn; Gore, Phoenix, AZ, USA) was positioned in the mesenteric artery, followed by antegrade periprosthetic high-density packed coiling of the aneurysm. The AOB remained excluded from mesenteric perfusion. The patient's clinical condition and abdominal contrast-enhanced multislice computed tomographic findings were unremarkable at the 9-year follow-up.</p><p><strong>Conclusion: </strong>The 9 year long-term efficacy in our case raises the possibility that perigraft coiling following stent-graft deployment in the SMA may represent a valuable technical option for large Bühler aneurysms that are not amenable to stand-alone coiling.</p>\",\"PeriodicalId\":52351,\"journal\":{\"name\":\"CVIR Endovascular\",\"volume\":\"7 1\",\"pages\":\"9\"},\"PeriodicalIF\":2.1000,\"publicationDate\":\"2024-01-10\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10781915/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"CVIR Endovascular\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1186/s42155-023-00416-4\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q3\",\"JCRName\":\"CARDIAC & CARDIOVASCULAR SYSTEMS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"CVIR Endovascular","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1186/s42155-023-00416-4","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
引用次数: 0
摘要
背景:布勒弧(AOB)是腹腔动脉(CA)和肠系膜上动脉(SMA)之间残留的胚胎吻合口。虽然通常无症状,但当腹腔动脉阻塞导致 SMA 和 CA 之间出现代偿性逆流,从而导致动脉瘤形成和出血时,它就具有临床意义。由于腹腔动脉瘤位于胰腺后深部,阻碍了开放手术,因此血管内旋转是主要的治疗方法:我们在此报告了一例 47 岁男性在摩托车外伤和脊椎手术后的康复过程中出现 2.8 厘米 AOB 囊状动脉瘤和腹腔干 LAM 压迫的病例。患者被认为不适合手术。由于 AOB 动脉瘤呈宽颈囊状,位于 SMA 和腹腔干底部之间,因此不适合采用传统的卷曲或裸金属支架和球囊辅助技术进行卷曲。为了将动脉瘤与 SMA 的直接流入排除在外,并进行安全有效的卷曲以排除逆行囊灌注,在肠系膜动脉中放置了一个 9 毫米的聚四氟乙烯支架移植物(Viabahn;戈尔公司,美国亚利桑那州凤凰城),然后对动脉瘤进行前向假体周围高密度填塞卷曲。AOB 仍被排除在肠系膜灌注之外。9 年随访期间,患者的临床状况和腹部对比增强多层计算机断层扫描结果均无异常:我们的病例经过 9 年的长期疗效证明,在 SMA 中部署支架移植物后进行移植物周围卷曲可能是治疗无法单独卷曲的大型布勒动脉瘤的一种有价值的技术选择。
Covered stent assisted coil embolization of large Buhler aneurysm in setting of chronic celiac trunk occlusion.
Background: The arc of Bühler (AOB) is a residual embryonal anastomosis between the celiac artery (CA) and the superior mesenteric artery (SMA). Although usually asymptomatic, it has clinical relevance when compensatory reverse flow between the SMA and the CA in response to celiac artery obstruction leads to aneurysm formation and bleeding. Endovascular coiling is the mainstay therapy because of the deep AOB retropancreatic location, which hinders open surgery.
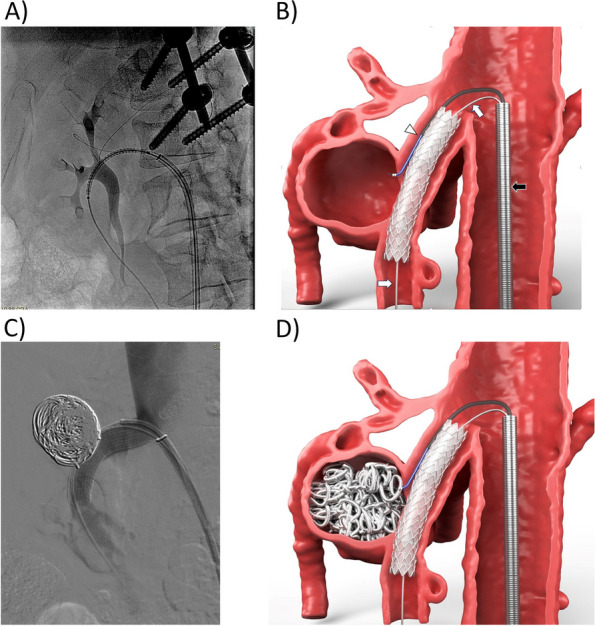
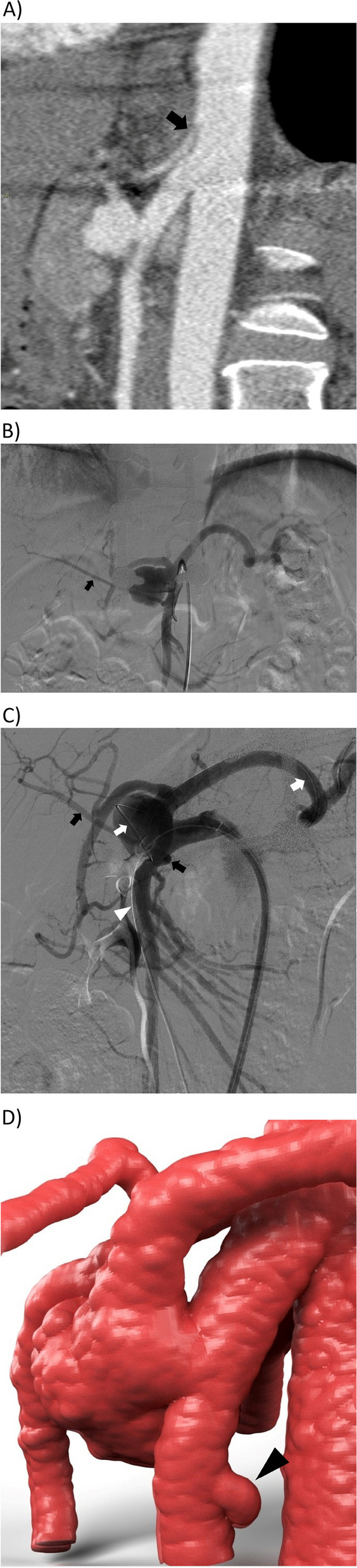
Case presentation: We herein report a case of a 2.8-cm AOB saccular aneurysm and LAM compression of celiac trunk in a 47-year-old man during rehabilitation following motorcycle trauma and vertebral surgery. The patient was considered unsuitable for surgery. Neither conventional coiling nor bare-metal stent and balloon-assisted techniques for coiling were suitable because of the wide necked saccular shape of AOB aneurysm interposed between the SMA and the floor of celiac trunk. To exclude the aneurysm from direct SMA inflow and permit safe and efficient coiling to rule out retrograde sac perfusion, a 9-mm polytetrafluoroethylene stent graft (Viabahn; Gore, Phoenix, AZ, USA) was positioned in the mesenteric artery, followed by antegrade periprosthetic high-density packed coiling of the aneurysm. The AOB remained excluded from mesenteric perfusion. The patient's clinical condition and abdominal contrast-enhanced multislice computed tomographic findings were unremarkable at the 9-year follow-up.
Conclusion: The 9 year long-term efficacy in our case raises the possibility that perigraft coiling following stent-graft deployment in the SMA may represent a valuable technical option for large Bühler aneurysms that are not amenable to stand-alone coiling.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
