Joey F H Reijmer, Lex D de Jong, Diederik H R Kempen, Mark P Arts, Job L C van Susante
{"title":"椎间活动度指标对决定在退行性脊椎滑脱症患者中增加器械融合的临床实用性","authors":"Joey F H Reijmer, Lex D de Jong, Diederik H R Kempen, Mark P Arts, Job L C van Susante","doi":"10.1097/BRS.0000000000004918","DOIUrl":null,"url":null,"abstract":"<p><strong>Study design: </strong>A prospective single-arm clinical study.</p><p><strong>Objective: </strong>To explore the clinical utility of an intervertebral motion metric by determining the proportion of patients for whom it changed their surgical treatment plan from decompression only to decompression with fusion or vice versa .</p><p><strong>Summary of background data: </strong>Lumbar spinal stenosis from degenerative spondylolisthesis is commonly treated with decompression only or decompression with additional instrumented fusion. An objective diagnostic tool capable of establishing abnormal motion between lumbar vertebrae to guide decision-making between surgical procedures is needed. To this end, a metric based on the vertebral sagittal plane translation-per-degree-of-rotation calculated from flexion-extension radiographs was developed.</p><p><strong>Materials and methods: </strong>First, spine surgeons documented their intended surgical plan. Subsequently, the participants' flexion-extension radiographs were taken. From these, the translation-per-degree-of-rotation was calculated and reported as a sagittal plane shear index (SPSI). The SPSI metric of the spinal level intended to be treated was used to decide if the intended surgical plan needed to be changed or not.</p><p><strong>Results: </strong>SPSI was determined for 75 participants. Of these, 51 (68%) had an intended surgical plan of decompression only and 24 (32%) had decompression with fusion. In 63% of participants, the SPSI was in support of their intended surgical plan. For 29% of participants, the surgeon changed the surgical plan after the SPSI metric became available to them. A suggested change in the surgical plan was overruled by 8% of participants. The final surgical plan was decompression only for 59 (79%) participants and decompression with fusion for 16 (21%) participants.</p><p><strong>Conclusion: </strong>The 29% change in intended surgical plans suggested that SPSI was considered by spine surgeons as an adjunct metric in deciding whether to perform decompression only or to add instrumented fusion. This change exceeded the a priori defined 15% considered necessary to show the potential clinical utility of SPSI.</p>","PeriodicalId":22193,"journal":{"name":"Spine","volume":" ","pages":"E355-E360"},"PeriodicalIF":3.7000,"publicationDate":"2024-11-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11458100/pdf/","citationCount":"0","resultStr":"{\"title\":\"Clinical Utility of an Intervertebral Motion Metric for Deciding on the Addition of Instrumented Fusion in Degenerative Spondylolisthesis.\",\"authors\":\"Joey F H Reijmer, Lex D de Jong, Diederik H R Kempen, Mark P Arts, Job L C van Susante\",\"doi\":\"10.1097/BRS.0000000000004918\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Study design: </strong>A prospective single-arm clinical study.</p><p><strong>Objective: </strong>To explore the clinical utility of an intervertebral motion metric by determining the proportion of patients for whom it changed their surgical treatment plan from decompression only to decompression with fusion or vice versa .</p><p><strong>Summary of background data: </strong>Lumbar spinal stenosis from degenerative spondylolisthesis is commonly treated with decompression only or decompression with additional instrumented fusion. An objective diagnostic tool capable of establishing abnormal motion between lumbar vertebrae to guide decision-making between surgical procedures is needed. To this end, a metric based on the vertebral sagittal plane translation-per-degree-of-rotation calculated from flexion-extension radiographs was developed.</p><p><strong>Materials and methods: </strong>First, spine surgeons documented their intended surgical plan. Subsequently, the participants' flexion-extension radiographs were taken. From these, the translation-per-degree-of-rotation was calculated and reported as a sagittal plane shear index (SPSI). The SPSI metric of the spinal level intended to be treated was used to decide if the intended surgical plan needed to be changed or not.</p><p><strong>Results: </strong>SPSI was determined for 75 participants. Of these, 51 (68%) had an intended surgical plan of decompression only and 24 (32%) had decompression with fusion. In 63% of participants, the SPSI was in support of their intended surgical plan. For 29% of participants, the surgeon changed the surgical plan after the SPSI metric became available to them. A suggested change in the surgical plan was overruled by 8% of participants. The final surgical plan was decompression only for 59 (79%) participants and decompression with fusion for 16 (21%) participants.</p><p><strong>Conclusion: </strong>The 29% change in intended surgical plans suggested that SPSI was considered by spine surgeons as an adjunct metric in deciding whether to perform decompression only or to add instrumented fusion. This change exceeded the a priori defined 15% considered necessary to show the potential clinical utility of SPSI.</p>\",\"PeriodicalId\":22193,\"journal\":{\"name\":\"Spine\",\"volume\":\" \",\"pages\":\"E355-E360\"},\"PeriodicalIF\":3.7000,\"publicationDate\":\"2024-11-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11458100/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Spine\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1097/BRS.0000000000004918\",\"RegionNum\":2,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2024/1/30 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q2\",\"JCRName\":\"CLINICAL NEUROLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Spine","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1097/BRS.0000000000004918","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/1/30 0:00:00","PubModel":"Epub","JCR":"Q2","JCRName":"CLINICAL NEUROLOGY","Score":null,"Total":0}
Clinical Utility of an Intervertebral Motion Metric for Deciding on the Addition of Instrumented Fusion in Degenerative Spondylolisthesis.
Study design: A prospective single-arm clinical study.
Objective: To explore the clinical utility of an intervertebral motion metric by determining the proportion of patients for whom it changed their surgical treatment plan from decompression only to decompression with fusion or vice versa .
Summary of background data: Lumbar spinal stenosis from degenerative spondylolisthesis is commonly treated with decompression only or decompression with additional instrumented fusion. An objective diagnostic tool capable of establishing abnormal motion between lumbar vertebrae to guide decision-making between surgical procedures is needed. To this end, a metric based on the vertebral sagittal plane translation-per-degree-of-rotation calculated from flexion-extension radiographs was developed.
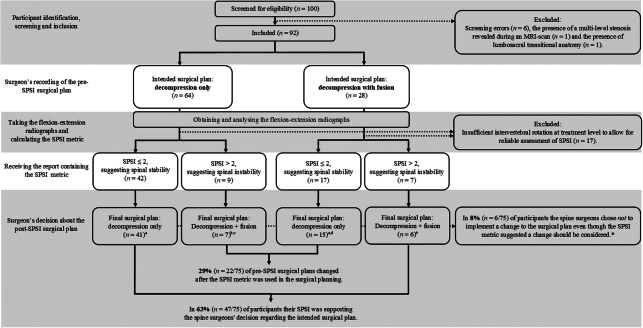
Materials and methods: First, spine surgeons documented their intended surgical plan. Subsequently, the participants' flexion-extension radiographs were taken. From these, the translation-per-degree-of-rotation was calculated and reported as a sagittal plane shear index (SPSI). The SPSI metric of the spinal level intended to be treated was used to decide if the intended surgical plan needed to be changed or not.
Results: SPSI was determined for 75 participants. Of these, 51 (68%) had an intended surgical plan of decompression only and 24 (32%) had decompression with fusion. In 63% of participants, the SPSI was in support of their intended surgical plan. For 29% of participants, the surgeon changed the surgical plan after the SPSI metric became available to them. A suggested change in the surgical plan was overruled by 8% of participants. The final surgical plan was decompression only for 59 (79%) participants and decompression with fusion for 16 (21%) participants.
Conclusion: The 29% change in intended surgical plans suggested that SPSI was considered by spine surgeons as an adjunct metric in deciding whether to perform decompression only or to add instrumented fusion. This change exceeded the a priori defined 15% considered necessary to show the potential clinical utility of SPSI.
期刊介绍:
Lippincott Williams & Wilkins is a leading international publisher of professional health information for physicians, nurses, specialized clinicians and students. For a complete listing of titles currently published by Lippincott Williams & Wilkins and detailed information about print, online, and other offerings, please visit the LWW Online Store.
Recognized internationally as the leading journal in its field, Spine is an international, peer-reviewed, bi-weekly periodical that considers for publication original articles in the field of Spine. It is the leading subspecialty journal for the treatment of spinal disorders. Only original papers are considered for publication with the understanding that they are contributed solely to Spine. The Journal does not publish articles reporting material that has been reported at length elsewhere.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
