{"title":"晚期前列腺癌患者的睾酮最低值与临床疗效:帕莫酸曲普瑞林III期研究的事后分析","authors":"Laurence Klotz, Tri Tat","doi":"10.1002/bco2.318","DOIUrl":null,"url":null,"abstract":"<div>\n \n \n <section>\n \n <h3> Objective</h3>\n \n <p>The objective of the study is to evaluate whether low nadir testosterone during treatment with triptorelin pamoate, a luteinising hormone-releasing hormone (LHRH) agonist, is associated with improved clinical outcomes in patients with advanced prostate cancer using a retrospective analysis of clinical trial data.</p>\n </section>\n \n <section>\n \n <h3> Patients and methods</h3>\n \n <p>Data were pooled from three prospective, 9–12-month Phase III studies of triptorelin monotherapy in patients with advanced prostate cancer (including NCT00751790). The serum testosterone concentration suppression targets evaluated were <0.35 nmol/L (<10 ng/dl), <0.7 nmol/L (<20 ng/dl), <1.7 nmol/L (<50 ng/dl) and ≥1.7 nmol/L. Overall survival (OS) and disease-specific survival (DSS) by testosterone suppression group were assessed by Kaplan–Meier analysis, with log-rank test. The time frame for the primary analysis was Days 1–518 (median OS follow-up 254 days [range, 29–518 days]) and for the sensitivity analyses was Days 1–262. Supplementary analyses combined the ≥0.7- to <1.7-nmol/L and ≥1.7-nmol/L groups.</p>\n </section>\n \n <section>\n \n <h3> Results</h3>\n \n <p>The sample size comprised 592 patients (most received triptorelin monotherapy; four reported concomitant androgen receptor-axis–targeted therapy). Nadir testosterones of <0.35, ≥0.35 to <0.7, ≥0.7 to <1.7 and ≥1.7 nmol/L were achieved by 96%, 3.2%, 0.34% and 0.17% of patients, respectively. Better OS with decreasing level of nadir testosterone was observed (<i>p</i> < 0.001) and this persisted after sensitivity/supplemental analyses (all <i>p</i> < 0.001). Differences in DSS with decreasing levels of nadir testosterone were not statistically significant in the primary analysis. Sensitivity/supplemental analysis showed better DSS with decreasing level of nadir testosterone (Days 1–262, <i>p</i> = 0.01; combined groups Days 1–518, <i>p</i> = 0.03; combined groups Days 1–262, <i>p</i> = 0.005).</p>\n </section>\n \n <section>\n \n <h3> Conclusion</h3>\n \n <p>Low nadir testosterone achieved during treatment with the LHRH agonist triptorelin was associated with improved OS and DSS in patients with advanced prostate cancer.</p>\n </section>\n </div>","PeriodicalId":72420,"journal":{"name":"BJUI compass","volume":"5 3","pages":"392-402"},"PeriodicalIF":1.9000,"publicationDate":"2024-01-10","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1002/bco2.318","citationCount":"0","resultStr":"{\"title\":\"Testosterone nadir and clinical outcomes in patients with advanced prostate cancer: Post hoc analysis of triptorelin pamoate Phase III studies\",\"authors\":\"Laurence Klotz, Tri Tat\",\"doi\":\"10.1002/bco2.318\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<div>\\n \\n \\n <section>\\n \\n <h3> Objective</h3>\\n \\n <p>The objective of the study is to evaluate whether low nadir testosterone during treatment with triptorelin pamoate, a luteinising hormone-releasing hormone (LHRH) agonist, is associated with improved clinical outcomes in patients with advanced prostate cancer using a retrospective analysis of clinical trial data.</p>\\n </section>\\n \\n <section>\\n \\n <h3> Patients and methods</h3>\\n \\n <p>Data were pooled from three prospective, 9–12-month Phase III studies of triptorelin monotherapy in patients with advanced prostate cancer (including NCT00751790). The serum testosterone concentration suppression targets evaluated were <0.35 nmol/L (<10 ng/dl), <0.7 nmol/L (<20 ng/dl), <1.7 nmol/L (<50 ng/dl) and ≥1.7 nmol/L. Overall survival (OS) and disease-specific survival (DSS) by testosterone suppression group were assessed by Kaplan–Meier analysis, with log-rank test. The time frame for the primary analysis was Days 1–518 (median OS follow-up 254 days [range, 29–518 days]) and for the sensitivity analyses was Days 1–262. Supplementary analyses combined the ≥0.7- to <1.7-nmol/L and ≥1.7-nmol/L groups.</p>\\n </section>\\n \\n <section>\\n \\n <h3> Results</h3>\\n \\n <p>The sample size comprised 592 patients (most received triptorelin monotherapy; four reported concomitant androgen receptor-axis–targeted therapy). Nadir testosterones of <0.35, ≥0.35 to <0.7, ≥0.7 to <1.7 and ≥1.7 nmol/L were achieved by 96%, 3.2%, 0.34% and 0.17% of patients, respectively. Better OS with decreasing level of nadir testosterone was observed (<i>p</i> < 0.001) and this persisted after sensitivity/supplemental analyses (all <i>p</i> < 0.001). Differences in DSS with decreasing levels of nadir testosterone were not statistically significant in the primary analysis. Sensitivity/supplemental analysis showed better DSS with decreasing level of nadir testosterone (Days 1–262, <i>p</i> = 0.01; combined groups Days 1–518, <i>p</i> = 0.03; combined groups Days 1–262, <i>p</i> = 0.005).</p>\\n </section>\\n \\n <section>\\n \\n <h3> Conclusion</h3>\\n \\n <p>Low nadir testosterone achieved during treatment with the LHRH agonist triptorelin was associated with improved OS and DSS in patients with advanced prostate cancer.</p>\\n </section>\\n </div>\",\"PeriodicalId\":72420,\"journal\":{\"name\":\"BJUI compass\",\"volume\":\"5 3\",\"pages\":\"392-402\"},\"PeriodicalIF\":1.9000,\"publicationDate\":\"2024-01-10\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://onlinelibrary.wiley.com/doi/epdf/10.1002/bco2.318\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"BJUI compass\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://bjui-journals.onlinelibrary.wiley.com/doi/10.1002/bco2.318\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q3\",\"JCRName\":\"UROLOGY & NEPHROLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"BJUI compass","FirstCategoryId":"1085","ListUrlMain":"https://bjui-journals.onlinelibrary.wiley.com/doi/10.1002/bco2.318","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"UROLOGY & NEPHROLOGY","Score":null,"Total":0}
Testosterone nadir and clinical outcomes in patients with advanced prostate cancer: Post hoc analysis of triptorelin pamoate Phase III studies
Objective
The objective of the study is to evaluate whether low nadir testosterone during treatment with triptorelin pamoate, a luteinising hormone-releasing hormone (LHRH) agonist, is associated with improved clinical outcomes in patients with advanced prostate cancer using a retrospective analysis of clinical trial data.
Patients and methods
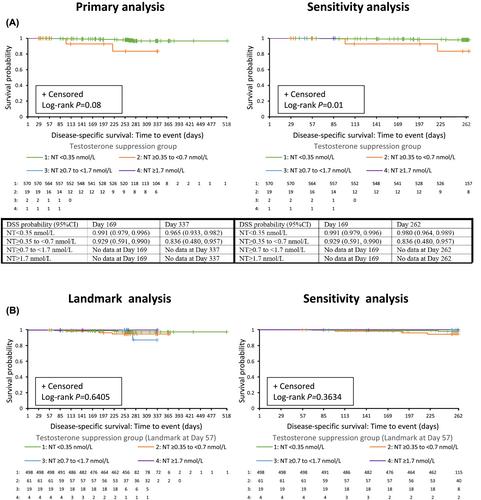
Data were pooled from three prospective, 9–12-month Phase III studies of triptorelin monotherapy in patients with advanced prostate cancer (including NCT00751790). The serum testosterone concentration suppression targets evaluated were <0.35 nmol/L (<10 ng/dl), <0.7 nmol/L (<20 ng/dl), <1.7 nmol/L (<50 ng/dl) and ≥1.7 nmol/L. Overall survival (OS) and disease-specific survival (DSS) by testosterone suppression group were assessed by Kaplan–Meier analysis, with log-rank test. The time frame for the primary analysis was Days 1–518 (median OS follow-up 254 days [range, 29–518 days]) and for the sensitivity analyses was Days 1–262. Supplementary analyses combined the ≥0.7- to <1.7-nmol/L and ≥1.7-nmol/L groups.
Results
The sample size comprised 592 patients (most received triptorelin monotherapy; four reported concomitant androgen receptor-axis–targeted therapy). Nadir testosterones of <0.35, ≥0.35 to <0.7, ≥0.7 to <1.7 and ≥1.7 nmol/L were achieved by 96%, 3.2%, 0.34% and 0.17% of patients, respectively. Better OS with decreasing level of nadir testosterone was observed (p < 0.001) and this persisted after sensitivity/supplemental analyses (all p < 0.001). Differences in DSS with decreasing levels of nadir testosterone were not statistically significant in the primary analysis. Sensitivity/supplemental analysis showed better DSS with decreasing level of nadir testosterone (Days 1–262, p = 0.01; combined groups Days 1–518, p = 0.03; combined groups Days 1–262, p = 0.005).
Conclusion
Low nadir testosterone achieved during treatment with the LHRH agonist triptorelin was associated with improved OS and DSS in patients with advanced prostate cancer.




 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
