Jorge Echeverri, Rui Martins, Kai Harenski, J Patrick Kampf, Paul McPherson, Julien Textoris, Jay L Koyner
{"title":"探索预测持续性严重急性肾损伤的生物标志物的成本效益:C-C Motif Chemokine Ligand 14 (CCL14)案例。","authors":"Jorge Echeverri, Rui Martins, Kai Harenski, J Patrick Kampf, Paul McPherson, Julien Textoris, Jay L Koyner","doi":"10.2147/CEOR.S434971","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Approximately 24% of hospitalized stage 2-3 acute kidney injury (AKI) patients will develop persistent severe AKI (PS-AKI), defined as KDIGO stage 3 AKI lasting ≥3 days or with death in ≤3 days or stage 2 or 3 AKI with dialysis in ≤3 days, leading to worse outcomes and higher costs. There is currently no consensus on an intervention that effectively reverts the course of AKI and prevents PS-AKI in the population with stage 2-3 AKI. This study explores the cost-utility of biomarkers predicting PS-AKI, under the assumption that such intervention exists by comparing C-C motif chemokine ligand 14 (CCL14) to hospital standard of care (SOC) alone.</p><p><strong>Methods: </strong>The analysis combined a 90-day decision tree using CCL14 operating characteristics to predict PS-AKI and clinical outcomes in 66-year-old patients, and a Markov cohort estimating lifetime costs and quality-adjusted life years (QALYs). Cost and QALYs from admission, 30-day readmission, intensive care, dialysis, and death were compared. Clinical and cost inputs were informed by a large retrospective cohort of US hospitals in the PINC AI Healthcare Database. Inputs and assumptions were challenged in deterministic and probabilistic sensitivity analyses. Two-way analyses were used to explore the efficacy and costs of an intervention preventing PS-AKI.</p><p><strong>Results: </strong>Depending on selected costs and early intervention efficacy, CCL14-directed care led to lower costs and more QALYs (dominating) or was cost-effective at the $50,000/QALY threshold. Assuming the intervention would avoid 10% of PS-AKI complications in AKI stage 2-3 patients identified as true positive resulted in 0.066 additional QALYs and $486 reduced costs. Results were robust to substantial parameter variation.</p><p><strong>Conclusion: </strong>The analysis suggests that in the presence of an efficacious intervention preventing PS-AKI, identifying people at risk using CCL14 in addition to SOC is likely to represent a cost-effective use of resources.</p>","PeriodicalId":47313,"journal":{"name":"ClinicoEconomics and Outcomes Research","volume":"16 ","pages":"1-12"},"PeriodicalIF":2.2000,"publicationDate":"2024-01-12","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10790637/pdf/","citationCount":"0","resultStr":"{\"title\":\"Exploring the Cost-Utility of a Biomarker Predicting Persistent Severe Acute Kidney Injury: The Case of C-C Motif Chemokine Ligand 14 (CCL14).\",\"authors\":\"Jorge Echeverri, Rui Martins, Kai Harenski, J Patrick Kampf, Paul McPherson, Julien Textoris, Jay L Koyner\",\"doi\":\"10.2147/CEOR.S434971\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Approximately 24% of hospitalized stage 2-3 acute kidney injury (AKI) patients will develop persistent severe AKI (PS-AKI), defined as KDIGO stage 3 AKI lasting ≥3 days or with death in ≤3 days or stage 2 or 3 AKI with dialysis in ≤3 days, leading to worse outcomes and higher costs. There is currently no consensus on an intervention that effectively reverts the course of AKI and prevents PS-AKI in the population with stage 2-3 AKI. This study explores the cost-utility of biomarkers predicting PS-AKI, under the assumption that such intervention exists by comparing C-C motif chemokine ligand 14 (CCL14) to hospital standard of care (SOC) alone.</p><p><strong>Methods: </strong>The analysis combined a 90-day decision tree using CCL14 operating characteristics to predict PS-AKI and clinical outcomes in 66-year-old patients, and a Markov cohort estimating lifetime costs and quality-adjusted life years (QALYs). Cost and QALYs from admission, 30-day readmission, intensive care, dialysis, and death were compared. Clinical and cost inputs were informed by a large retrospective cohort of US hospitals in the PINC AI Healthcare Database. Inputs and assumptions were challenged in deterministic and probabilistic sensitivity analyses. Two-way analyses were used to explore the efficacy and costs of an intervention preventing PS-AKI.</p><p><strong>Results: </strong>Depending on selected costs and early intervention efficacy, CCL14-directed care led to lower costs and more QALYs (dominating) or was cost-effective at the $50,000/QALY threshold. Assuming the intervention would avoid 10% of PS-AKI complications in AKI stage 2-3 patients identified as true positive resulted in 0.066 additional QALYs and $486 reduced costs. Results were robust to substantial parameter variation.</p><p><strong>Conclusion: </strong>The analysis suggests that in the presence of an efficacious intervention preventing PS-AKI, identifying people at risk using CCL14 in addition to SOC is likely to represent a cost-effective use of resources.</p>\",\"PeriodicalId\":47313,\"journal\":{\"name\":\"ClinicoEconomics and Outcomes Research\",\"volume\":\"16 \",\"pages\":\"1-12\"},\"PeriodicalIF\":2.2000,\"publicationDate\":\"2024-01-12\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10790637/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"ClinicoEconomics and Outcomes Research\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.2147/CEOR.S434971\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2024/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q3\",\"JCRName\":\"HEALTH CARE SCIENCES & SERVICES\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"ClinicoEconomics and Outcomes Research","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.2147/CEOR.S434971","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/1/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"HEALTH CARE SCIENCES & SERVICES","Score":null,"Total":0}
Exploring the Cost-Utility of a Biomarker Predicting Persistent Severe Acute Kidney Injury: The Case of C-C Motif Chemokine Ligand 14 (CCL14).
Background: Approximately 24% of hospitalized stage 2-3 acute kidney injury (AKI) patients will develop persistent severe AKI (PS-AKI), defined as KDIGO stage 3 AKI lasting ≥3 days or with death in ≤3 days or stage 2 or 3 AKI with dialysis in ≤3 days, leading to worse outcomes and higher costs. There is currently no consensus on an intervention that effectively reverts the course of AKI and prevents PS-AKI in the population with stage 2-3 AKI. This study explores the cost-utility of biomarkers predicting PS-AKI, under the assumption that such intervention exists by comparing C-C motif chemokine ligand 14 (CCL14) to hospital standard of care (SOC) alone.
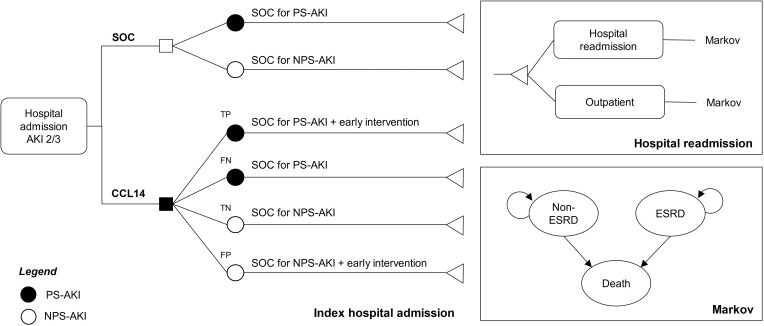
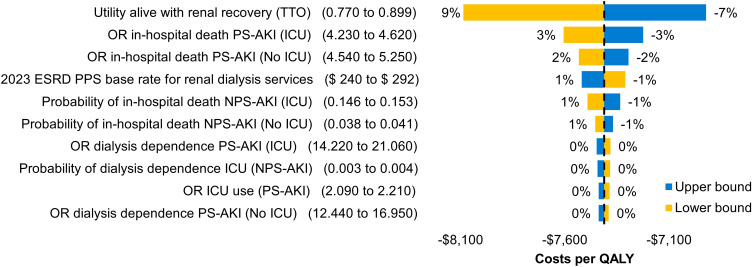
Methods: The analysis combined a 90-day decision tree using CCL14 operating characteristics to predict PS-AKI and clinical outcomes in 66-year-old patients, and a Markov cohort estimating lifetime costs and quality-adjusted life years (QALYs). Cost and QALYs from admission, 30-day readmission, intensive care, dialysis, and death were compared. Clinical and cost inputs were informed by a large retrospective cohort of US hospitals in the PINC AI Healthcare Database. Inputs and assumptions were challenged in deterministic and probabilistic sensitivity analyses. Two-way analyses were used to explore the efficacy and costs of an intervention preventing PS-AKI.
Results: Depending on selected costs and early intervention efficacy, CCL14-directed care led to lower costs and more QALYs (dominating) or was cost-effective at the $50,000/QALY threshold. Assuming the intervention would avoid 10% of PS-AKI complications in AKI stage 2-3 patients identified as true positive resulted in 0.066 additional QALYs and $486 reduced costs. Results were robust to substantial parameter variation.
Conclusion: The analysis suggests that in the presence of an efficacious intervention preventing PS-AKI, identifying people at risk using CCL14 in addition to SOC is likely to represent a cost-effective use of resources.





 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
