Aleksandar Pavlovic, Ljubica Sedlar, Katarina Lazarevic, Jelica Vukmirovic, Tarik Plojovic, Ksenija Mijovic, Dragan Vasin, Dragan Masulovic
{"title":"纵隔并发感染并伴有主动脉食管瘘--X 射线和计算机断层扫描成像","authors":"Aleksandar Pavlovic, Ljubica Sedlar, Katarina Lazarevic, Jelica Vukmirovic, Tarik Plojovic, Ksenija Mijovic, Dragan Vasin, Dragan Masulovic","doi":"10.1002/ird3.49","DOIUrl":null,"url":null,"abstract":"<p>Aortoesophageal fistula is a rare, but life-threatening complication of several conditions [<span>1, 2</span>]. Computed tomography (CT) angiography is the diagnostic modality of choice [<span>3, 4</span>]. There is no consensus on therapeutic strategy [<span>1</span>].</p><p>A 73-year-old woman presented with severe chest pain and pressure, shortness of breath, and sweating. She also had a fever and low blood pressure. During observation, she began vomiting blood, lost consciousness, and became hemodynamically unstable. Chest X-ray showed mediastinal widening with a suspected aneurysm of the thoracic aorta and gas outlining the mediastinal structures, suggestive of pneumomediastinum (Figure 1).</p><p>CT angiography revealed mediastinal fat stranding, edema, fluid collections, and free gas inclusion. In the differential diagnosis, esophageal perforation with mediastinitis was assumed, but an infectious aneurysm was also considered due to the periaortic gas distribution (Figure 2). There were no previous data in the patient's history and anamnestic or imaging findings. Extensive gas locules around the esophagus were highly suggestive of esophageal perforation (Figure 2a). The esophagus was filled with hemorrhagic content, while the thoracic aorta was aneurysmally dilated, with irregular contours, overlayed by a thickened esophageal wall, with contrast extravasation into the lumen, clearly indicating an aortoesophageal fistula (Figure 2b,d).</p><p>Recurrent hematemesis and deterioration of the patient's condition unfortunately led to a fatal outcome, without surgery. Chest pain and progressive hematemesis are typical clinical signs of fistula [<span>4</span>]. Earlier indication of CT angiography could possibly increase the chances of survival [<span>2</span>]. Digital subtraction angiography could also clearly confirm the contrast extravasation [<span>3</span>]. Para-aortic fat stranding and fluid, as well as periaortic gas, may raise the suspicion of an infected aortic aneurysm [<span>5</span>]. Although we cannot determine the source of infection in this case with certainty, the presence of an aortoesophageal fistula was clearly demonstrated radiologically.</p><p><b>Aleksandar Pavlovic</b>: Conceptualization (Equal); data curation (equal); methodology (equal); visualization (equal); writing—original draft (lead). <b>Ljubica Sedlar</b>: Conceptualization (equal); formal analysis (equal); investigation (equal); methodology (equal); validation (equal); visualization (equal); writing—review and editing (lead). <b>Katarina Lazarevic</b>: Conceptualization (equal); formal analysis (equal); methodology (equal). <b>Jelica Vukmirovic</b>: Conceptualization (equal); methodology (equal). <b>Tarik Plojovic</b>: Data curation (equal); formal analysis (equal); methodology (equal); writing—original draft (supporting). <b>Ksenija Mijovic</b>: Conceptualization (equal); investigation (equal); methodology (equal); writing—original draft (supporting). <b>Dragan Vasin</b>: Conceptualization (equal); methodology (equal); project administration (equal); supervision (equal); validation (equal); writing—review and editing (equal). <b>Dragan Masulovic</b>: Supervision (lead); validation (lead).</p><p>The authors declare no conflicts of interest.</p><p>This article is a practice-oriented case study description. As such, the creation of this case study article did not involve any formal research study, and IRB review was not required for this article.</p><p>Not applicable.</p>","PeriodicalId":73508,"journal":{"name":"iRadiology","volume":"2 1","pages":"96-98"},"PeriodicalIF":0.0000,"publicationDate":"2024-01-12","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1002/ird3.49","citationCount":"0","resultStr":"{\"title\":\"Complicated infection in the mediastinum with aortoesophageal fistula—X-ray and computed tomography imaging\",\"authors\":\"Aleksandar Pavlovic, Ljubica Sedlar, Katarina Lazarevic, Jelica Vukmirovic, Tarik Plojovic, Ksenija Mijovic, Dragan Vasin, Dragan Masulovic\",\"doi\":\"10.1002/ird3.49\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p>Aortoesophageal fistula is a rare, but life-threatening complication of several conditions [<span>1, 2</span>]. Computed tomography (CT) angiography is the diagnostic modality of choice [<span>3, 4</span>]. There is no consensus on therapeutic strategy [<span>1</span>].</p><p>A 73-year-old woman presented with severe chest pain and pressure, shortness of breath, and sweating. She also had a fever and low blood pressure. During observation, she began vomiting blood, lost consciousness, and became hemodynamically unstable. Chest X-ray showed mediastinal widening with a suspected aneurysm of the thoracic aorta and gas outlining the mediastinal structures, suggestive of pneumomediastinum (Figure 1).</p><p>CT angiography revealed mediastinal fat stranding, edema, fluid collections, and free gas inclusion. In the differential diagnosis, esophageal perforation with mediastinitis was assumed, but an infectious aneurysm was also considered due to the periaortic gas distribution (Figure 2). There were no previous data in the patient's history and anamnestic or imaging findings. Extensive gas locules around the esophagus were highly suggestive of esophageal perforation (Figure 2a). The esophagus was filled with hemorrhagic content, while the thoracic aorta was aneurysmally dilated, with irregular contours, overlayed by a thickened esophageal wall, with contrast extravasation into the lumen, clearly indicating an aortoesophageal fistula (Figure 2b,d).</p><p>Recurrent hematemesis and deterioration of the patient's condition unfortunately led to a fatal outcome, without surgery. Chest pain and progressive hematemesis are typical clinical signs of fistula [<span>4</span>]. Earlier indication of CT angiography could possibly increase the chances of survival [<span>2</span>]. Digital subtraction angiography could also clearly confirm the contrast extravasation [<span>3</span>]. Para-aortic fat stranding and fluid, as well as periaortic gas, may raise the suspicion of an infected aortic aneurysm [<span>5</span>]. Although we cannot determine the source of infection in this case with certainty, the presence of an aortoesophageal fistula was clearly demonstrated radiologically.</p><p><b>Aleksandar Pavlovic</b>: Conceptualization (Equal); data curation (equal); methodology (equal); visualization (equal); writing—original draft (lead). <b>Ljubica Sedlar</b>: Conceptualization (equal); formal analysis (equal); investigation (equal); methodology (equal); validation (equal); visualization (equal); writing—review and editing (lead). <b>Katarina Lazarevic</b>: Conceptualization (equal); formal analysis (equal); methodology (equal). <b>Jelica Vukmirovic</b>: Conceptualization (equal); methodology (equal). <b>Tarik Plojovic</b>: Data curation (equal); formal analysis (equal); methodology (equal); writing—original draft (supporting). <b>Ksenija Mijovic</b>: Conceptualization (equal); investigation (equal); methodology (equal); writing—original draft (supporting). <b>Dragan Vasin</b>: Conceptualization (equal); methodology (equal); project administration (equal); supervision (equal); validation (equal); writing—review and editing (equal). <b>Dragan Masulovic</b>: Supervision (lead); validation (lead).</p><p>The authors declare no conflicts of interest.</p><p>This article is a practice-oriented case study description. As such, the creation of this case study article did not involve any formal research study, and IRB review was not required for this article.</p><p>Not applicable.</p>\",\"PeriodicalId\":73508,\"journal\":{\"name\":\"iRadiology\",\"volume\":\"2 1\",\"pages\":\"96-98\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2024-01-12\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://onlinelibrary.wiley.com/doi/epdf/10.1002/ird3.49\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"iRadiology\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://onlinelibrary.wiley.com/doi/10.1002/ird3.49\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"iRadiology","FirstCategoryId":"1085","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1002/ird3.49","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
Complicated infection in the mediastinum with aortoesophageal fistula—X-ray and computed tomography imaging
Aortoesophageal fistula is a rare, but life-threatening complication of several conditions [1, 2]. Computed tomography (CT) angiography is the diagnostic modality of choice [3, 4]. There is no consensus on therapeutic strategy [1].
A 73-year-old woman presented with severe chest pain and pressure, shortness of breath, and sweating. She also had a fever and low blood pressure. During observation, she began vomiting blood, lost consciousness, and became hemodynamically unstable. Chest X-ray showed mediastinal widening with a suspected aneurysm of the thoracic aorta and gas outlining the mediastinal structures, suggestive of pneumomediastinum (Figure 1).
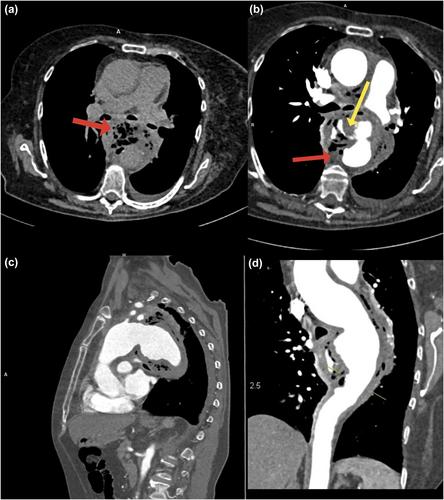
CT angiography revealed mediastinal fat stranding, edema, fluid collections, and free gas inclusion. In the differential diagnosis, esophageal perforation with mediastinitis was assumed, but an infectious aneurysm was also considered due to the periaortic gas distribution (Figure 2). There were no previous data in the patient's history and anamnestic or imaging findings. Extensive gas locules around the esophagus were highly suggestive of esophageal perforation (Figure 2a). The esophagus was filled with hemorrhagic content, while the thoracic aorta was aneurysmally dilated, with irregular contours, overlayed by a thickened esophageal wall, with contrast extravasation into the lumen, clearly indicating an aortoesophageal fistula (Figure 2b,d).
Recurrent hematemesis and deterioration of the patient's condition unfortunately led to a fatal outcome, without surgery. Chest pain and progressive hematemesis are typical clinical signs of fistula [4]. Earlier indication of CT angiography could possibly increase the chances of survival [2]. Digital subtraction angiography could also clearly confirm the contrast extravasation [3]. Para-aortic fat stranding and fluid, as well as periaortic gas, may raise the suspicion of an infected aortic aneurysm [5]. Although we cannot determine the source of infection in this case with certainty, the presence of an aortoesophageal fistula was clearly demonstrated radiologically.
This article is a practice-oriented case study description. As such, the creation of this case study article did not involve any formal research study, and IRB review was not required for this article.



 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
