Hauke Schneider, Jan Meis, Christina Klose, Peter Ratzka, Wolf-Dirk Niesen, David B Seder, Julian Bösel
{"title":"严重脑卒中患者的手术与扩张气管造口术:SETPOINT2 后期分析。","authors":"Hauke Schneider, Jan Meis, Christina Klose, Peter Ratzka, Wolf-Dirk Niesen, David B Seder, Julian Bösel","doi":"10.1007/s12028-023-01933-9","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Tracheostomy in mechanically ventilated patients with severe stroke can be performed surgically or dilationally. Prospective data comparing both methods in patients with stroke are scarce. The randomized Stroke-Related Early Tracheostomy vs Prolonged Orotracheal Intubation in Neurocritical Care Trial2 (SETPOINT2) assigned 382 mechanically ventilated patients with stroke to early tracheostomy versus extubation or standard tracheostomy. Surgical tracheostomy (ST) was performed in 41 of 307 SETPOINT2 patients, and the majority received dilational tracheostomy (DT). We aimed to compare ST and DT in these patients with patients.</p><p><strong>Methods: </strong>All SETPOINT2 patients with ST were compared with a control group of patients with stroke undergoing DT (1:2), selected by propensity score matching that included the factors stroke type, SETPOINT2 randomization group, Stroke Early Tracheostomy score, patient age, and premorbid functional status. Successful decannulation was the primary outcome, and secondary outcome parameters included functional outcome at 6 months and adverse events attributable to tracheostomy. Potential predictors of decannulation were evaluated by regression analysis.</p><p><strong>Results: </strong>Baseline characteristics were comparable in the two groups of patients with stroke undergoing ST (n = 41) and matched patients with stroke undergoing DT (n = 82). Tracheostomy was performed significantly later in the ST group than in the DT group (median 9 [interquartile range {IQR} 5-12] vs. 9 [IQR 4-11] days after intubation, p = 0.025). Patients with ST were mechanically ventilated longer (median 19 [IQR 17-24] vs.14 [IQR 11-19] days, p = 0.008) and stayed in the intensive care unit longer (median 23 [IQR 16-27] vs. 17 [IQR 13-24] days, p = 0.047), compared with patients with DT. The intrahospital infection rate was significantly higher in the ST group compared to the DT group (14.6% vs. 1.2%, p = 0.002). At 6 months, decannulation rates (56% vs. 61%), functional outcomes, and mortality were not different. However, decannulation was performed later in the ST group compared to the DT group (median 81 [IQR 66-149] vs. 58 [IQR 32-77] days, p = 0.004). Higher baseline Stroke Early Tracheostomy score negatively predicted decannulation.</p><p><strong>Conclusions: </strong>In ventilated patients with severe stroke in need of tracheostomy, surgical and dilational methods are associated with comparable decannulation rate and functional outcome at 6 months. However, ST was associated with longer time to decannulation and higher rates of early infections, supporting the dilational approach to tracheostomy in ventilated patients with stroke.</p>","PeriodicalId":19118,"journal":{"name":"Neurocritical Care","volume":" ","pages":"146-155"},"PeriodicalIF":4.2000,"publicationDate":"2024-08-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11335838/pdf/","citationCount":"0","resultStr":"{\"title\":\"Surgical Versus Dilational Tracheostomy in Patients with Severe Stroke: A SETPOINT2 Post hoc Analysis.\",\"authors\":\"Hauke Schneider, Jan Meis, Christina Klose, Peter Ratzka, Wolf-Dirk Niesen, David B Seder, Julian Bösel\",\"doi\":\"10.1007/s12028-023-01933-9\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Tracheostomy in mechanically ventilated patients with severe stroke can be performed surgically or dilationally. Prospective data comparing both methods in patients with stroke are scarce. The randomized Stroke-Related Early Tracheostomy vs Prolonged Orotracheal Intubation in Neurocritical Care Trial2 (SETPOINT2) assigned 382 mechanically ventilated patients with stroke to early tracheostomy versus extubation or standard tracheostomy. Surgical tracheostomy (ST) was performed in 41 of 307 SETPOINT2 patients, and the majority received dilational tracheostomy (DT). We aimed to compare ST and DT in these patients with patients.</p><p><strong>Methods: </strong>All SETPOINT2 patients with ST were compared with a control group of patients with stroke undergoing DT (1:2), selected by propensity score matching that included the factors stroke type, SETPOINT2 randomization group, Stroke Early Tracheostomy score, patient age, and premorbid functional status. Successful decannulation was the primary outcome, and secondary outcome parameters included functional outcome at 6 months and adverse events attributable to tracheostomy. Potential predictors of decannulation were evaluated by regression analysis.</p><p><strong>Results: </strong>Baseline characteristics were comparable in the two groups of patients with stroke undergoing ST (n = 41) and matched patients with stroke undergoing DT (n = 82). Tracheostomy was performed significantly later in the ST group than in the DT group (median 9 [interquartile range {IQR} 5-12] vs. 9 [IQR 4-11] days after intubation, p = 0.025). Patients with ST were mechanically ventilated longer (median 19 [IQR 17-24] vs.14 [IQR 11-19] days, p = 0.008) and stayed in the intensive care unit longer (median 23 [IQR 16-27] vs. 17 [IQR 13-24] days, p = 0.047), compared with patients with DT. The intrahospital infection rate was significantly higher in the ST group compared to the DT group (14.6% vs. 1.2%, p = 0.002). At 6 months, decannulation rates (56% vs. 61%), functional outcomes, and mortality were not different. However, decannulation was performed later in the ST group compared to the DT group (median 81 [IQR 66-149] vs. 58 [IQR 32-77] days, p = 0.004). Higher baseline Stroke Early Tracheostomy score negatively predicted decannulation.</p><p><strong>Conclusions: </strong>In ventilated patients with severe stroke in need of tracheostomy, surgical and dilational methods are associated with comparable decannulation rate and functional outcome at 6 months. However, ST was associated with longer time to decannulation and higher rates of early infections, supporting the dilational approach to tracheostomy in ventilated patients with stroke.</p>\",\"PeriodicalId\":19118,\"journal\":{\"name\":\"Neurocritical Care\",\"volume\":\" \",\"pages\":\"146-155\"},\"PeriodicalIF\":4.2000,\"publicationDate\":\"2024-08-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11335838/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Neurocritical Care\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1007/s12028-023-01933-9\",\"RegionNum\":3,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2024/1/30 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q2\",\"JCRName\":\"CLINICAL NEUROLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Neurocritical Care","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1007/s12028-023-01933-9","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/1/30 0:00:00","PubModel":"Epub","JCR":"Q2","JCRName":"CLINICAL NEUROLOGY","Score":null,"Total":0}
Surgical Versus Dilational Tracheostomy in Patients with Severe Stroke: A SETPOINT2 Post hoc Analysis.
Background: Tracheostomy in mechanically ventilated patients with severe stroke can be performed surgically or dilationally. Prospective data comparing both methods in patients with stroke are scarce. The randomized Stroke-Related Early Tracheostomy vs Prolonged Orotracheal Intubation in Neurocritical Care Trial2 (SETPOINT2) assigned 382 mechanically ventilated patients with stroke to early tracheostomy versus extubation or standard tracheostomy. Surgical tracheostomy (ST) was performed in 41 of 307 SETPOINT2 patients, and the majority received dilational tracheostomy (DT). We aimed to compare ST and DT in these patients with patients.
Methods: All SETPOINT2 patients with ST were compared with a control group of patients with stroke undergoing DT (1:2), selected by propensity score matching that included the factors stroke type, SETPOINT2 randomization group, Stroke Early Tracheostomy score, patient age, and premorbid functional status. Successful decannulation was the primary outcome, and secondary outcome parameters included functional outcome at 6 months and adverse events attributable to tracheostomy. Potential predictors of decannulation were evaluated by regression analysis.
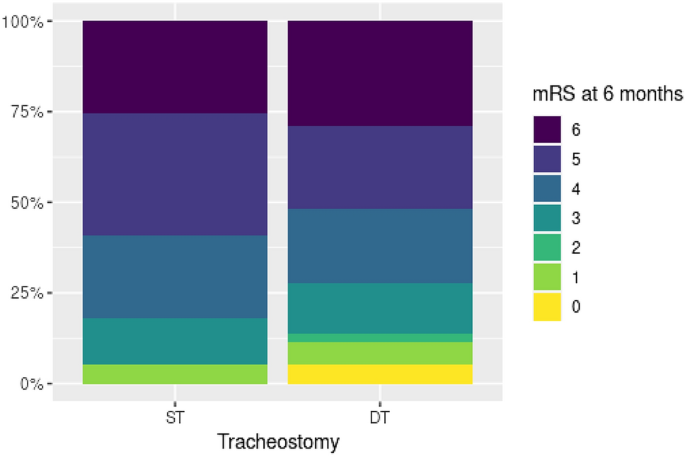
Results: Baseline characteristics were comparable in the two groups of patients with stroke undergoing ST (n = 41) and matched patients with stroke undergoing DT (n = 82). Tracheostomy was performed significantly later in the ST group than in the DT group (median 9 [interquartile range {IQR} 5-12] vs. 9 [IQR 4-11] days after intubation, p = 0.025). Patients with ST were mechanically ventilated longer (median 19 [IQR 17-24] vs.14 [IQR 11-19] days, p = 0.008) and stayed in the intensive care unit longer (median 23 [IQR 16-27] vs. 17 [IQR 13-24] days, p = 0.047), compared with patients with DT. The intrahospital infection rate was significantly higher in the ST group compared to the DT group (14.6% vs. 1.2%, p = 0.002). At 6 months, decannulation rates (56% vs. 61%), functional outcomes, and mortality were not different. However, decannulation was performed later in the ST group compared to the DT group (median 81 [IQR 66-149] vs. 58 [IQR 32-77] days, p = 0.004). Higher baseline Stroke Early Tracheostomy score negatively predicted decannulation.
Conclusions: In ventilated patients with severe stroke in need of tracheostomy, surgical and dilational methods are associated with comparable decannulation rate and functional outcome at 6 months. However, ST was associated with longer time to decannulation and higher rates of early infections, supporting the dilational approach to tracheostomy in ventilated patients with stroke.
期刊介绍:
Neurocritical Care is a peer reviewed scientific publication whose major goal is to disseminate new knowledge on all aspects of acute neurological care. It is directed towards neurosurgeons, neuro-intensivists, neurologists, anesthesiologists, emergency physicians, and critical care nurses treating patients with urgent neurologic disorders. These are conditions that may potentially evolve rapidly and could need immediate medical or surgical intervention. Neurocritical Care provides a comprehensive overview of current developments in intensive care neurology, neurosurgery and neuroanesthesia and includes information about new therapeutic avenues and technological innovations. Neurocritical Care is the official journal of the Neurocritical Care Society.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
