Elena W. Y. Hsieh, Alexandre Bolze, Joseph D. Hernandez
{"title":"先天性免疫错误阐明了人类免疫学的机制,并为精准医疗铺平了道路。","authors":"Elena W. Y. Hsieh, Alexandre Bolze, Joseph D. Hernandez","doi":"10.1111/imr.13311","DOIUrl":null,"url":null,"abstract":"<p>The <span><b><i>Yellow Brick Road</i></b></span> leads Dorothy through Oz to the Emerald City—a luminescent green metropolis where she hopes to meet the great and powerful Wizard. The Emerald City is the destination of Dorothy's journey, where desires become reality. Arguably, the <span><b><i>“Emerald City”</i></b></span> for most physician-scientists caring for patients with inborn errors of immunity (IEI) is to apply effective therapies that target the specific impaired cell type/pathway, while avoiding detrimental effects on the rest of the immune system and other tissues (Figure 1). That is, <b><i>to use the right treatment, at the right time, for the right patient</i></b>—precision medicine at its best. The journey to this Emerald City has always started with the patient's symptoms and history. However, the constellation of these clinical clues has significantly changed over time, making it more challenging to begin the odyssey down the yellow brick road. In 1952, Dr. Ogden Bruton started his journey with patients who had recurrent pneumonias. Along the road, he found that they lacked serum γ-globulins. He then discovered a causative single gene defect, inherited as a Mendelian trait with full penetrance. Finally, he arrived at the targeted destination of immunoglobulin replacement therapy.<span><sup>1</sup></span> Today, neither the starting point nor the road that follows are as straight and smooth.</p><p>As <i>Bucciol</i> et al. (1) describe in this issue, the wide availability and application of next-generation sequencing (NGS) methods, particularly whole exome/genome sequencing (WES/WGS), has significantly increased “the discovery rate” of additional IEI. The most recent International Union of Immunological Societies update (2022) included 55 novel monogenic gene defects, and one phenocopy due to autoantibodies discovered since January 2020, bringing the total number of IEI to 485.<span><sup>2</sup></span> In some cases, distinct pathogenic variants at the same locus cause different IEI phenotypes (allelic heterogeneity; <b><i>one gene, many phenotypes</i></b>). In other cases, pathogenic variants in different genes governing one common pathway cause the same IEI (locus heterogeneity; <b><i>many genes, one phenotype</i></b>).<span><sup>3</sup></span> Furthermore, as <i>Vinh</i> (2) discusses, IEI can also exemplify <b><i>non</i>-<i>Mendelian basis of disease</i></b>. While the overwhelming majority of IEI have been identified and mechanistically deciphered as monogenic, there are increasing reports of oligogenic IEI syndromes,<span><sup>4-8</sup></span> wherein lesions in two or more distinct genes contribute to a clinical phenotype that has some features of the corresponding monogenic IEI disorders. Somatic mosaic mutations may lead to a milder or a more severe form of the disease, which may be influenced by the known pathogenicity of the mutation at the germline level.<span><sup>9</sup></span> Alterations in gene expression such as DNA methylation and epigenetic modifications can also result in IEI. These new IEI expand beyond traditional boundaries, as recurrent infections are neither the only nor the most common clinical presentation. Clinical phenotypes as diverse as autoimmunity/inflammation, lymphoproliferation, malignancy, and severe allergy, involving multiple organs,<span><sup>10</sup></span> have certainly expanded the breadth of IEI across medical and scientific fields. Consequently, the field of IEI has now adopted a <span><b><i>“flying monkey's perspective”</i></b></span> that now includes clinical subspecialties, where genetic etiology is not traditionally a cornerstone of the diagnostic work up. As we, clinical immunologists, strive to collaborate with other subspecialists to advocate for the importance of genetic testing and help with the interpretation of results, challenges surrounding cost and accessibility may deter genetic evaluation. We and others have published genetic testing recommendation guidelines<span><sup>11</sup></span> to support the diagnostic odyssey and reduce delays in treatment.</p><p>Now, <b><i>with great power comes great responsibility</i></b>—while use of WES/WGS has led to the discovery of many new IEI and confers the <i>power</i> to “quickly” diagnose rare disease (completed in a clinical lab in days to weeks), it also often reveals the much-dreaded list of <i>variants of unknown significance</i> or VUS. Raising the questions—Who should establish if a VUS impairs a specific immune process and identify the associated phenotype, <i>a.k.a functional validation</i>? Who should fund this work? How long will it take? And do we wait until we have proven causality to determine a treatment course? The answer is it depends. When VUS are found in genes known to be associated with IEI, validation may involve evaluating protein expression or more complex cellular functional analyses (via clinical studies or research protocols). For VUS in genes not previously associated with IEI, first there is a “triage” process to decide whether further work up should be pursued. Once “triaged,” functional validation of these VUS typically requires lengthy and labor-intensive research evaluations necessary to prove causality—which are not compatible with “real time” clinical decision making. Hence, novel technologies are required to improve the “triage” and evaluation processes—making a case for deep immune profiling.<span><sup>12</sup></span> <i>Hurabeille</i> et al. (3) review emerging genomic tools to functionally assess candidate genetic variants. <b><i>Functional genomics</i></b> aims to understand the relationship between an organism's genome and its phenotype, which often display a hierarchical nature from molecular to organ-specific manifestations. High-throughput approaches to produce genetic variants, either with synthetic DNA sequences or direct endogenous genome editing has opened exciting avenues to study coding variants biochemically or using cell-based assays—improving speed of functional validation. In the era of WGS, noncoding variants are increasingly appearing, and their study necessitates a shift from the starting point of predictable amino acid consequence as can be determined in coding variants. <i>Hurabeille</i> et al. review how to determine the functional consequences of noncoding variants (i) utilizing natural genetic variation and CRISPR/Cas9 cellular engineering models, (ii) assessing chromatin accessibility, and (iii) applying multiplexed single-cell multiomic approaches.</p><p>The IEI landscape today is quite different from that in 1952…As Dorothy would say, <span><b><i>“Toto, I've a feeling we're not in Kansas anymore”.</i></b></span> Although the discovery and characterization of IEI have become more complex in the intervening decades, we summarize below how the reviews in this issue illustrate how IEI continue to illuminate mechanisms of human immunology (Figure 2).</p><p>The genetic theory of infectious disease formulated in the 1920s attempted to set the stage for a link between genes and immunity. But it was not until 1939, when Karl Diehl's and Otmar von Verschuer's studies of tuberculosis in monozygotic and dizygotic twins suggested that genetic factors contributed to tuberculosis susceptibility. Since then, several IEI underlying Mendelian Susceptibility of Mycobacterial Disease have been discovered;<span><sup>13</sup></span> along with many other monogenic defects that reveal specific mechanisms of antimicrobial immunity. Though the genetic determinants of antimicrobial immunity were not spotlighted until the 1950s, the function of human immune cells in combating infectious organisms were highlighted in the early 1900s. Nobel awards to Metchnikoff and Ehrlich in 1908 showcased the importance of phagocytosis in immunity. Metchnikoff even went on to postulate that intracellular digestion is important to maintain a balance between host intestinal immunity and microbiota—a founding principle of why phagocyte defects may present with (sometimes very early onset) inflammatory bowel disease (IBD), as discussed in <i>Zerbe</i> et al. (4) In their review, the authors describe different genetic <b><i>neutrophil defects</i></b> as paradigms of pathways critical to bacterial and antifungal immunity and IBD. While the infectious complications and antimicrobial prophylactic and/or treatment regimens for these IEI are similar, the underlying mechanisms of their autoinflammatory complications are distinct. Hence, a “precision medicine” approach to their inflammatory conditions requires the genetic diagnosis.</p><p>Neutrophil defects are not the only IEI that have enlightened <b><i>antifungal immunity</i></b>. <i>Vinh</i> (2) showed how the major molecular leap in understanding chronic mucocutaneous candidiasis (CMC) came with the genetic discovery of dominant-negative mutations in signal transducer and activator of transcription (STAT)3 in autosomal-dominant hyper-IgE syndrome (AD-HIES, also known as Job's syndrome).<span><sup>14, 15</sup></span> From this, it was deduced that defects in the T helper-producing interleukin (IL)-17 (Th17) subset of T cells, caused by the mutant STAT3, underlie CMC. Grounded on the principle of pathophysiologic homogeneity, this Th17 finding was a “pillar” that enabled the identification of numerous other IEI marked by CMC, converging on defective IL-17-based responses.<span><sup>16-21</sup></span> In their review, <i>Asano</i> et al. (5) focus on STAT1 gain-of-function (GOF), which accounts for approximately 50% of the genetic causality of CMC. STAT1 GOF patients show lower proportion of Th17 cells suggesting impaired differentiation.<span><sup>22</sup></span> Further support for the central role of the IL-17 axis in the immunopathogenesis of CMC is the correlation between this infection and the presence of neutralizing auto-antibodies (auto-Abs) to these mediators (IL-17A, IL-17, IL-22), as in autoimmune polyendocrinopathy-candidiasis-ectodermal dystrophy (APECED) or in CMC-affected thymoma patients,<span><sup>23, 24</sup></span> reviewed in <i>Vinh</i> (2) and <i>Bastard</i> et al (6). Moreover, production of such auto-Abs has been found to precede the infection, suggesting a causal role in the mycosis, rather than a consequence. Identifying the underlying etiology, whether it be a monogenic defect or a result of auto-Ab pathogenicity, determines distinct treatment paradigms, and once again highlights the importance of understanding the underlying immunogenetic mechanism in guiding precision medicine.</p><p>IEI patients with unique clinical infectious symptomatology have also enlightened mechanisms of <b><i>antiviral immunity</i></b>. <i>Gonench</i> et al. (7) review how viral infections may present with unusual manifestations with atypical or compensatory inflammatory responses. They particularly highlight how the vaccine strain of rubella virus can cause inflammatory granulomas in the skin and sometimes other tissues. The time between inoculation and pathogenic effects can be between three weeks and decades. Rates of virus-associated malignancies are also increased in patients with IEI. With these various complications, viral infections represent a significant source of morbidity in patients with IEI. Targeted cellular antiviral therapies borrowed from hematopoietic bone marrow transplant (HSCT) research are currently being applied to treat chronic viremia in IEI with specific viral susceptibility.<span><sup>25, 26</sup></span></p><p>The best-known case of IEI in popular culture is that of David Vetter (1971–1983), who had severe combined immunodeficiency (SCID) and lived in a sterile isolator for 12 years, known as the “bubble boy.” Since then, the <b><i>SCID diagnostic</i>, <i>genetic etiology</i>, <i>and treatment landscape</i></b> has dramatically changed as reviewed in <i>Aranda</i> et al. (8) Currently, 19 different genetic causes have been identified.<span><sup>2</sup></span> Yet, for some (~6–10%)<span><sup>27</sup></span> there is no known genetic basis. We can expect that this percentage will decrease yearly as additional IEI are discovered. For example, our group recently described how a hypomorphic LCK variant led to a SCID phenotype with autoinflammatory complications.<span><sup>28</sup></span> Newborn screening (NBS) has led to decreased morbidity and mortality, as patients are diagnosed soon after birth and HSCT can be pursued prior to occurrence of infectious complications. Furthermore, advances in gene therapy reviewed by <i>Kohn</i> et al. (9) and <i>Porteus</i> et al. (10) pave the road for precision medicine with curative goals for SCID.</p><p>As the number of causative genetic etiologies of SCID increased with NBS, so did our understanding of critical pathways in lymphocyte development, particularly T cells, as congenital athymia diagnoses also benefited from NBS. We and others describe how SCID NBS has helped reveal the true prevalence and socioeconomic burden of congenital athymia,<span><sup>29-31</sup></span> supporting the eventual FDA approval of thymic implantation. <i>Dinges</i> et al. (11) review <b><i>primary and secondary defects in the thymus</i></b>, which include natural aging and resultant thymic atrophy. The thymus is the primary site of T-cell development, enabling the generation and selection of a diverse T-cell repertoire that recognizes nonself, yet remains tolerant to self-antigens. Thymic output has been shown to be inversely correlated with the incidence of infections and cancer.<span><sup>32</sup></span> Hence, thymus defects lead to increased risk of infection, autoimmunity, and malignancy. Immunological outcomes of thymus removal in infancy (a byproduct of corrective surgery for congenital heart defects) and adulthood (i.e., thymoma, myasthenia gravis, etc.) have corroborated these findings. Thymectomized (young adult) patients demonstrate a decrease in naïve T-cell populations, T-cell oligoclonality, and increased expression of senescence markers—essentially T-cell phenotypes correlated with increased autoimmunity, malignancy, and mortality in the elderly.<span><sup>33, 34</sup></span></p><p>IEI associated with <b><i>thymic stromal defects</i></b> include those related to syndromes resulting from defective embryological processes that encompass structures of the midline, and specific genes critical to thymic development. For example, defects in forkhead box (FOX)N1, long appreciated as the cause of SCID in nude mice, have been recently identified as an IEI leading to congenital athymia in humans. FOXN1 is a member of the forkhead/winged helix family of transcription factors that controls the development, differentiation, and survival of skin epithelial cells and cortical and medullary thymic epithelial cells (mTECs) both during embryogenesis and in post-natal life. FOXN1 biallelic loss-of-function (LOF) and heterozygous LOF, demonstrate varying degrees of T-cell lymphopenia, infections, and autoimmunity, exemplifying the <i>one gene, different phenotypes</i> model and demonstrating the critical role of FOXN1 in different stages of T-cell development.<span><sup>35</sup></span> In their review, <i>Bastard</i> et al. (6) also show how different IEI affecting <b><i>central T</i>-<i>cell tolerance</i></b> illuminate the mechanism of <b><i>development of auto</i>-<i>Abs that neutralize type I interferon (IFN)</i></b>.<span><sup>36-38</sup></span> For example, more than 80% of patients with IEI in the alternative NF-kB pathway carry neutralizing auto-Abs to type I IFN.<span><sup>39</sup></span> In these patients, thymus structure is abnormal and expression of AIRE, a critical regulator of central T-cell tolerance, is impaired in mTECs. Auto-Ab neutralization of type I IFN persisted even after HSCT in these patients, further demonstrating that mTEC-intrinsic deficiency of AIRE underlies the development of auto-Abs against type I IFN, and ultimately predisposes patients to multiple viral infections.</p><p>In 1965, Bruce Glick and his colleagues wrote about their “suspicion regarding the importance of the bursa in antibody production.” Robert Good and Max Cooper revisited the role of the bursa and thymus in chickens and published an article in 1966 in the Journal of Experimental Medicine, where they showed that B (bursa-derived) cells are required for antibody responses, whereas T (thymus-derived) cells mediate delayed-type hypersensitivity reactions, such as graft-versus-host rejection.<span><sup>40</sup></span> Max Cooper, a pediatrician and clinical immunologist, went on to make a set of clinical observations about these two lineages. Boys with Wiskott–Aldrich syndrome developed widespread herpes viral lesions, yet had high levels of antibodies. In contrast, boys with agammaglobunemia could control viral infections even if they lacked antibody responses.<span><sup>41</sup></span></p><p><i>Tangye</i> et al. (12) review how IEI have illuminated <b><i>B</i>-<i>cell function and roles in immunological memory and host protection</i>, <i>as well as allergic disease</i></b>, through the lens of HIES due to STAT3 defects. <i>Tangye</i> et al. (12) take us on a journey that begins with the first demonstration, that germline heterozygous LOF/dominant negative (DN) mutations in STAT3 caused AD-HIES (2007), followed by the discovery of other genetic disorders in the IL-6 and IL-21 cytokine signaling pathways, which revealed the roles of each of these proteins in B-cell survival, isotype switching, and memory formation. For example, the function of ZNF341 has largely been elucidated by studies examining HIES patients, establishing its important role in regulating STAT3 expression and autoinduction.<span><sup>42-44</sup></span> <i>Tangye</i> et al. also discuss how studies of HIES have revealed aspects of (i) the interplay between STATs, (ii) the cytokines (and their signaling pathways) that are required for B-cell development and generation of long-lived humoral immunity and memory, and (iii) IL-6/STAT3 pathway defects and their role in dysregulated IgE production in IEI.</p><p>B-cell dysfunction in IEI has historically been associated with common variable immunodeficiency (CVID). <i>Romberg</i> et al. (13) review how <b><i>genetic variability</i>, <i>epigenetic changes</i>, <i>tolerogenic defects</i>, <i>and dysbiosis contribute to CVID heterogeneity</i></b>. The authors review the pathophysiology of CVID due to primary and secondary defects in B-cell activation, B-cell survival, regulatory T cell (Treg) dysfunction, B-cell tolerance, and aberrant germinal center (GC) dynamics. Their studies of malignancy-free excisional lymph node biopsies from CVID patients reveal that CVID GCs can either be diminutive or exuberantly hyperplastic and asymmetric. Correlation of these tissues with paired blood samples show that patients with hyperplastic GCs have the lowest serum IgA concentrations, the highest serum endotoxin concentrations, and invariably experience noninfectious complications, specifically autoimmune cytopenias. In contrast, patients manifesting only sinopulmonary infectious complications primarily display hypoplastic GCs. Our research group has also described peripheral blood immunological phenotypes involving T- and B-cell receptor signaling pathways, that best correlate with noninfectious outcomes in CVID, such as granulomatous lymphocytic interstitial lung disease.<span><sup>45</sup></span> Future validation of these findings may carry therapeutic ramifications for our ability to predict, which CVID patients will develop noninfectious complications.</p><p>This T–B cell interaction discussed in <i>Romberg</i> et al. (13) is also visited by <i>Borna</i> et al. (14) who review how Tregs may play a critical role in B-cell development including repertoire, and regulation of autoreactive (silenced) B cells in the periphery. Patients with IPEX have a transitional BCR repertoire that is similar to healthy individuals, whereas they have a mature naïve BCR repertoire that is enriched in autoreactive cells. Furthermore, autoreactive BCR repertoires are associated with other T-cell defects and silenced following gene therapy for T-cell defects. Taken together, these observations imply that Tregs may play a critical role in reducing numbers of autoreactive B cells in the periphery.</p><p>Patients characterized by noninfectious episodes of inflammation, but lacking high-titer autoantibodies or autoantigen-reactive T cells have violated the established dogma of autoreactivity.<span><sup>46, 47</sup></span> In the late 20th century, these disorders were termed <b><i>autoinflammatory syndromes</i></b> to distinguish them from autoimmune disorders. They were characterized molecularly by the identification of the genes whose defects caused four landmark hereditary periodic fever syndromes: TNF receptor super family member 1A (TNFRSF1A) in TNFR1-associated periodic syndromes (TRAPS), pyrin (MEFV) in familial Mediterranean fever, mevalonate kinase (MVK) in Hyper-IgD syndrome, and NLR pyrin domain containing 3 (NLRP3) in cryopyrin-associated autoinflammatory syndrome (CAPS). The group of contributing physician scientists in <i>Putnam</i> et al. (15) review NLRP3 inflammasome biology, a journey of discovery, which started from a case report in 1940 and led to the meeting of five families and 69 individuals with a lifelong history of cold-induced rash, fever, and arthralgias. The NLRP3 gene was cloned in 2001, followed by unraveling inflammasome biology including intracellular stress that triggers NLRP3 activation, genotype/phenotype associations in monogenic disease, protein structural analyses, mouse models of disease, and reaching their goal of targeted therapy with monoclonal antibodies that block IL-1 and IL-18, instigators of the patients' symptomatology.</p><p>Pathogenic variants perturbing proteasome molecules collectively known as <b><i>Proteasome associated autoinflammatory syndromes</i> (<i>PRAAS</i>)</b> result in proteasome deficiency and subsequent accumulation of ubiquitinated proteins. This pathologic build-up of proteins leads to unfolded protein response (UPR) that causes the expression of type I IFN genes. Hence, PRAAS are often considered a subclass of type I interferonopathy. <i>Poli</i> (16) reviews different IEI that underlie PRAAS, and the central role of proteasomes in cellular apoptotic function and immune response. Not surprisingly, defects in proteasomes lead to an increased IFN signature, and have been linked to autoimmune disease (such as lupus, myositis, or Sjogren syndrome) thereby exemplifying how molecular understanding of rare diseases exposes shared mechanisms with more common disorders. This <b>“<i>rare</i>-<i>to</i>-<i>common</i>” <i>paradigm</i></b> is also illustrated in <b><i>Down syndrome</i> (<i>DS</i>)</b> whereby insights from type I interferonopathies can be applied to our understanding of immunological implications of the most common genetic disorder associated with intellectual disability. <i>Ramba</i> et al. (17) review the clinical manifestations of increased infections and autoimmunity in DS, and how they are explained by specific immune cellular phenotypic and/or functional abnormalities. These abnormalities stem from increased type I and II IFN signaling due to increased IFN receptor expression (four out of six of the IFN receptor genes reside on chromosome 21). Along with the Espinosa lab, we have described in detail the downstream cellular effects of this increased interferon signature, along with multiple immunological and extra immunological manifestations associated with such cellular abnormalities.<span><sup>48, 49</sup></span> In fact, these clinical immunological and nonimmunological phenotypes of individuals with DS overlap with those of patients with STAT1 GOF or STAT3 GOF, implicating this pathway in a wide array of DS manifestations.<span><sup>50, 51</sup></span></p><p>Indeed, <i>Asano</i> et al. (5) review how <b><i>STAT1 GOF</i></b> results in the overproduction of IFN-α/β, IFN-γ, and IL-27, leading to immunodeficiency, autoimmunity, and/or cerebral aneurysm, among other complications. In contrast, Largent et al. recently demonstrated that it is the dysregulation of IFN-γ signaling in STAT1 GOF that promotes phenotypes associated with autoimmunity. They showed that STAT1 GOF autoimmunity is characterized by adaptive immune activation due to the dysregulation of STAT1 signaling through both type I and type II IFN receptors. Furthermore, they found that Stat1 GOF mice without type I IFN receptors were partially protected from STAT1-driven systemic inflammation, whereas the depletion of type II IFN receptors abrogated autoimmune manifestations. These results offer an intriguing new perspective on the relationship between IFN and STAT1 GOF, suggesting that activation via the IFN-γ receptor, rather than type I IFN, is essential for STAT1-dependent immune tolerance failure. This same concept is reviewed by <i>Chaimowitz</i> et al. (18) who extend the review to other JAK/STAT defects, their negative regulators' defects, and their causative roles in immune dysregulation, along with treatment choices in these disorders. Defects in JAK/STAT signaling provide another example of <i>one gene, multiple phenotypes</i>. IEI of STAT1 can be classified in four types of disease: autosomal recessive (AR) complete LOF, AR partial LOF, AD LOF, and AD GOF.<span><sup>52-56</sup></span> <i>Chaimowitz</i> et al. (18) review the body of literature describing the use of JAK inhibition in IEI resulting in JAK/STAT GOF phenotypes, type I interferonopathy, and PRAAS.</p><p>Monogenic disorders that impact Treg cell function or survival, are collectively called <b><i><b>Tregopathies</b></i></b>. <i>Borna</i> et al. (14) review the first Tregopathy disorder discovered, FOXP3 deficiency or IPEX. IPEX patients may present with normal T-cell count to low numbers of Tregs. In IPEX, the conventional memory T cells are usually increased as compared to the naïve subset and are skewed toward Th2 and/or Th17 over Th1 phenotype. <i>Borna</i> et al. (14) review how these T-cell subsets drive organ-specific autoimmunity, and how comparison of methylation and phenotypes suggests that Tregs in patients with IPEX may be somewhat plastic, becoming inflammatory T cells. Hence, pharmacological, or cellular therapeutic approaches to improve Treg numbers or function constitute a prime example of precision medicine in IEI. Not surprisingly, as the number of novel IEI recognized has increased, so have the genetic etiologies underlying Tregopathies, including IL-2Rβ defects described by our and the Lenardo groups in 2019.<span><sup>57-60</sup></span> Common presentations of these disorders include very early onset (VEO)-IBD, as reviewed by <i>Hall</i> et al. (19) To date, 80 monogenic causes of VEO-IBD have been identified and published. <i>Hall</i> et al. (19) review the different immunological pathways described in VEO-IBD and the burgeoning personalized therapy developing in this area.</p><p>Dr. Ogden not only described the first IEI, but he set the foundation for the first glimpse at precision medicine—the life-saving innovation of gamma globulin replacement therapy that has added decades to the lives of patients with humoral immune deficiencies. Since then, new generations of antimicrobials used prophylactically and/or therapeutically have reduced life-threatening fungal, bacterial, and viral infections in IEI. Autoimmune/inflammatory complications of IEI have historically been managed with nonspecific immunosuppression, such as glucocorticoids, cyclosporine, mycophenolate mofetil, etc. Advancements in the understanding of immune mechanisms of rheumatologic diseases led to the development and application of novel targeted therapeutics, including small molecule inhibitors, fusion proteins, and other biologics. These were <b><i>then</i> “<i>borrowed</i>” <i>and used for the treatment of IEI that involve aspects of autoimmunity</i>, <i>lymphoproliferation</i>, <i>and malignancy</i></b>.</p><p>For example, JAK inhibitors (JAKinibs) have proven effective in the treatment of rheumatoid arthritis (RA) and other immune mediated diseases,<span><sup>61</sup></span> and this paved the way for their use to treat immune dysregulation in patients with STAT1 and STAT3 GOF, as reviewed by <i>Chaimowitz</i> et al. (18) and <i>Asano</i> et al. (5) JAKinibs have also been used in type I interferonopathies as reviewed by <i>Ramba</i> et al. (17) and <i>Poli</i> (16). <i>Chaimowitz</i> et al. (18) review how tocilizumab, a humanized anti-IL-6 receptor monoclonal antibody that binds to soluble and membrane bound IL-6 receptors, has shown promise in the treatment of RA, and most recently STAT3 GOF. <i>Putnam</i> et al. (15) review how IL-1 blockade used in RA and systemic juvenile idiopathic arthritis (sJIA) have been used to treat CAPS. Abatacept, a soluble protein comprised of the extracellular domain of CTLA-4 linked to the Fc portion of IgG1 used in RA,<span><sup>62</sup></span> was also “borrowed” for use in CTLA-4 haploinsufficiency and LRBA deficiency.<span><sup>63-65</sup></span> In contrast, ipilimumab, an anti-CTLA-4 monoclonal antibody used to treat advanced stage melanoma, can “iatrogenically induce” the clinical autoimmune symptomatology of patients with CTLA-4 haploinsufficiency. We have published on the inverse correlation between the CTLA4 mRNA levels and degree of CTLA-4 pathway disruption, regardless of the etiology (genetic or iatrogenic).<span><sup>66</sup></span> Taken together, the mechanism of action of abatacept, ipilimumab, and the immunopathology of patients with CTLA-4 haploinsufficiency, reveal the relationship between rare diseases and common pathways in autoimmunity and malignancy.</p><p>Some of the challenges surrounding novel therapeutics specifically designed and approved for IEI are exacerbated by the rarity of these disorders, but we are beginning to see a “turning of the tide.” <i>Jordan</i> (20) reviews the pathophysiology, genetic etiologies, and targeted therapy development for patients with hemophagocytic lymphohistiocytosis (HLH) specifically. HLH is best conceptualized as a maladaptive state of excessive T-cell activation driving life-threatening myeloid cell activation, largely via IFNγ. The discovery of the key role of IFNγ in HLH pathogenesis in multiple murine models of HLH by independent laboratories spurred the clinical development of the neutralizing anti-IFNγ monoclonal antibody called emapalumab for use in patients with HLH. This development occurred relatively rapidly, taking only 14 years from initial publication of the therapeutic target to FDA approval of a clinical drug in 2020. Development and application of this therapy was unique in involving a number of firsts: the first trial of rationally targeted therapy in HLH, the first trial conducted per good clinical practice standards (or with industry sponsorship) in this disease entity, and the first drug ever approved by a regulatory agency for patients with HLH.</p><p>The use of these agents for the treatment of common autoimmune disorders exemplified the reduced scope of side effects, one of the main goals of precision medicine. But the “borrowed” indication of these agents to treat rare IEI best illustrated the concept of targeting the specific molecular basis of an immunologic disorder. JAKinibs inhibit the excessive activation of the JAK/STAT pathway in patients with STAT1/3 GOF, abatacept provides CTLA-4 to patients with CTLA-4 and LRBA deficiency who lack this T-cell activation inhibitory protein, IL-1 blockade neutralizes the downstream effects of the pro-inflammatory cytokines that patients with CAPS produce in excess. <b><i>These represent</i>, “<i>the right treatment for the right patient</i>.”</b> <i>But what about the</i> “<i>right time</i>?” Arguably, the “right time” to implement a treatment is to prevent end-organ damage effects, which is challenging in IEI given the common delay in diagnosis. In the advent of NBS for SCID, curative therapy via HSCT can now be implemented prior to development of life-threatening infections. And while HSCT is not exactly precise, it is still first line curative therapy in IEI until restoration of normal gene function via <b><i>gene therapy</i></b> approaches reach “prime time.” There have been both scientific and regulatory challenges along this road as highlighted by <i>Kohn</i> (9) and <i>Ghanim</i> et al. (10).</p><p>Traditionally, gene therapy approaches for IEI were attempted through gene addition using <b><i>retroviral or lentiviral vectors</i></b>. Although this has the advantage of sustained gene expression without requiring specific targeting by the vector, disadvantages, including lack of precise control over copy numbers and risk of random integration with possibility of leukemogenesis, placed gene therapy for X-linked SCID and CGD on hold for many years.<span><sup>67</sup></span> Early experience in gene therapy for adenosine deaminase (ADA) highlighted the critical importance of reconstituted cells having a selective advantage in success of the therapy—which sets the foundation for the higher success rate of HSCT for LOF disorders vs. GOF. With the shift of technology to lentiviral vector use, improvements in (i) cell culture and transduction efficiency cells, (ii) control over vector integration, and (iii) vector cryopreservation have made gene therapy more feasible for a greater number of patients, with a growing number of treated ADA patients demonstrating long term immune reconstitution. Gene therapy for ADA SCID has been approved by European regulators, however, the challenge of making definitive therapies for rare diseases commercially viable remains a major obstacle in reaching this goal.</p><p>Given the known serious complications in treating some IEI with gene addition approaches and advances in gene editing with <b><i>CRISPR</i>-<i>Cas9 technology</i></b>, many therapies are now focused on <b><i>correcting endogenous genes</i></b> as reviewed by <i>Ghanim</i> et al. (10) The major advantage of this approach is that endogenous regulation of gene expression is preserved—allowing normal expression during immune cell development and function. <i>Ghanim</i> et al. (10) illustrate the advantages of gene correction in several IEI, including B-cell tyrosine kinase (<i>BTK</i>), <i>CYBB, and FOXP3</i>. The challenge with gene editing approaches for personalized medicine will be in adapting approaches to ensure that they will benefit more than individual patients, or in achieving a new regulatory framework that is more permissive of personalized adaptation of therapies. Although gene therapy typically targets hematopoietic stem cells for a lasting cure, <i><b>targeting the pathologic cells is an alternative strategy</b>. Ghanim</i> et al (10). and <i>Borna</i> et al. (14), review one such strategy for replacing Tregs in IPEX. Autologous effector T cells can be transduced by a lentiviral vector expressing wild type FOXP3, which effectively transforms the cells to Tregs. This therapeutic approach is currently undergoing clinical trial. As cellular therapies continue to develop in oncology such the use of chimeric antigen receptor (CAR) T cells for lymphoma, and virus-specific T cells in HSCT, they will likely also be “borrowed” for treatment of IEI, and hopefully further illuminate mechanisms of pathway specific therapy.</p><p>What have IEI illuminated in human immunology since 1952? IEI are not as rare as we thought, but as a field we still need to undertake large collaborative efforts to follow the yellow brick road and reach the Emerald city. There is as much strength in publications from large numbers of patients from a multidisciplinary group, as there is from single patient case reports/research articles—a single grain of rice can tip the balance in our favor. While the toolbox to decipher novel IEI and dissect the causative molecular underpinnings of antimicrobial immunity and self-tolerance has expanded, so has the diversity of “flavors” of genetic etiologies in IEI. Encountering a variant in a known disease-related gene is not synonymous with pathogenicity. While experimental validation with either traditional immunological assays or high throughput variant functionalization approaches are still the gold standard to prove causation, they are labor intensive, often equating to a graduate student thesis and/or postdoctoral fellowship project, and hence not on clinically actionable timeline. Collaboration and sharing of data are still the most effective way to advance our understanding of human immunology, and importantly, help our patients.</p><p>Data sharing supports the ability to develop and apply machine learning methods, and thereby predict functional consequences. Perhaps, ChatGPT will replace researchers in IEI one day, but that day is not today. The advances in commercial machine learning that are reducing the costs of statistical prediction are simultaneously increasing the value of data (which enable prediction) and judgment (which determines why prediction matters). However, in IEI, when a patient does not “fit” the clinical picture typically seen for a given genetic disorder, instead of “judging the fit” we inquire “why does it not fit?” As long as we remain curious, and not judgmental, we academic physician-scientists stand a chance of keeping our jobs and not becoming an endangered species.</p><p>While we focus on gathering the data along the yellow brick road to the Emerald City of precise supportive and curative approaches in IEI (Figure 1), we must worry about the other “green” along the way; the for-profit biologic and cellular/gene therapy market is not always accessible to our “ultra-rare” patients. As we raise awareness of IEI across medical specialties outside of clinical immunology, we will likely gain visibility across pharmaceutical industry, NIH agencies, and FDA governance. Following the <i><b>yellow brick road</b></i> is not without challenges, but, just like Dorothy, we hopefully bring our <i><b>brains (scarecrow), heart (tinman), and courage (lion)</b></i> to help along the way.</p><p>This work was supported by the Jeffrey Modell Foundation Primary Immunodeficiency Center at Children's Hospital Colorado.</p><p>The author has no conflicts of interest to declare.</p>","PeriodicalId":178,"journal":{"name":"Immunological Reviews","volume":"322 1","pages":"5-14"},"PeriodicalIF":8.3000,"publicationDate":"2024-02-02","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1111/imr.13311","citationCount":"0","resultStr":"{\"title\":\"Inborn errors of immunity illuminate mechanisms of human immunology and pave the road to precision medicine\",\"authors\":\"Elena W. Y. Hsieh, Alexandre Bolze, Joseph D. Hernandez\",\"doi\":\"10.1111/imr.13311\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p>The <span><b><i>Yellow Brick Road</i></b></span> leads Dorothy through Oz to the Emerald City—a luminescent green metropolis where she hopes to meet the great and powerful Wizard. The Emerald City is the destination of Dorothy's journey, where desires become reality. Arguably, the <span><b><i>“Emerald City”</i></b></span> for most physician-scientists caring for patients with inborn errors of immunity (IEI) is to apply effective therapies that target the specific impaired cell type/pathway, while avoiding detrimental effects on the rest of the immune system and other tissues (Figure 1). That is, <b><i>to use the right treatment, at the right time, for the right patient</i></b>—precision medicine at its best. The journey to this Emerald City has always started with the patient's symptoms and history. However, the constellation of these clinical clues has significantly changed over time, making it more challenging to begin the odyssey down the yellow brick road. In 1952, Dr. Ogden Bruton started his journey with patients who had recurrent pneumonias. Along the road, he found that they lacked serum γ-globulins. He then discovered a causative single gene defect, inherited as a Mendelian trait with full penetrance. Finally, he arrived at the targeted destination of immunoglobulin replacement therapy.<span><sup>1</sup></span> Today, neither the starting point nor the road that follows are as straight and smooth.</p><p>As <i>Bucciol</i> et al. (1) describe in this issue, the wide availability and application of next-generation sequencing (NGS) methods, particularly whole exome/genome sequencing (WES/WGS), has significantly increased “the discovery rate” of additional IEI. The most recent International Union of Immunological Societies update (2022) included 55 novel monogenic gene defects, and one phenocopy due to autoantibodies discovered since January 2020, bringing the total number of IEI to 485.<span><sup>2</sup></span> In some cases, distinct pathogenic variants at the same locus cause different IEI phenotypes (allelic heterogeneity; <b><i>one gene, many phenotypes</i></b>). In other cases, pathogenic variants in different genes governing one common pathway cause the same IEI (locus heterogeneity; <b><i>many genes, one phenotype</i></b>).<span><sup>3</sup></span> Furthermore, as <i>Vinh</i> (2) discusses, IEI can also exemplify <b><i>non</i>-<i>Mendelian basis of disease</i></b>. While the overwhelming majority of IEI have been identified and mechanistically deciphered as monogenic, there are increasing reports of oligogenic IEI syndromes,<span><sup>4-8</sup></span> wherein lesions in two or more distinct genes contribute to a clinical phenotype that has some features of the corresponding monogenic IEI disorders. Somatic mosaic mutations may lead to a milder or a more severe form of the disease, which may be influenced by the known pathogenicity of the mutation at the germline level.<span><sup>9</sup></span> Alterations in gene expression such as DNA methylation and epigenetic modifications can also result in IEI. These new IEI expand beyond traditional boundaries, as recurrent infections are neither the only nor the most common clinical presentation. Clinical phenotypes as diverse as autoimmunity/inflammation, lymphoproliferation, malignancy, and severe allergy, involving multiple organs,<span><sup>10</sup></span> have certainly expanded the breadth of IEI across medical and scientific fields. Consequently, the field of IEI has now adopted a <span><b><i>“flying monkey's perspective”</i></b></span> that now includes clinical subspecialties, where genetic etiology is not traditionally a cornerstone of the diagnostic work up. As we, clinical immunologists, strive to collaborate with other subspecialists to advocate for the importance of genetic testing and help with the interpretation of results, challenges surrounding cost and accessibility may deter genetic evaluation. We and others have published genetic testing recommendation guidelines<span><sup>11</sup></span> to support the diagnostic odyssey and reduce delays in treatment.</p><p>Now, <b><i>with great power comes great responsibility</i></b>—while use of WES/WGS has led to the discovery of many new IEI and confers the <i>power</i> to “quickly” diagnose rare disease (completed in a clinical lab in days to weeks), it also often reveals the much-dreaded list of <i>variants of unknown significance</i> or VUS. Raising the questions—Who should establish if a VUS impairs a specific immune process and identify the associated phenotype, <i>a.k.a functional validation</i>? Who should fund this work? How long will it take? And do we wait until we have proven causality to determine a treatment course? The answer is it depends. When VUS are found in genes known to be associated with IEI, validation may involve evaluating protein expression or more complex cellular functional analyses (via clinical studies or research protocols). For VUS in genes not previously associated with IEI, first there is a “triage” process to decide whether further work up should be pursued. Once “triaged,” functional validation of these VUS typically requires lengthy and labor-intensive research evaluations necessary to prove causality—which are not compatible with “real time” clinical decision making. Hence, novel technologies are required to improve the “triage” and evaluation processes—making a case for deep immune profiling.<span><sup>12</sup></span> <i>Hurabeille</i> et al. (3) review emerging genomic tools to functionally assess candidate genetic variants. <b><i>Functional genomics</i></b> aims to understand the relationship between an organism's genome and its phenotype, which often display a hierarchical nature from molecular to organ-specific manifestations. High-throughput approaches to produce genetic variants, either with synthetic DNA sequences or direct endogenous genome editing has opened exciting avenues to study coding variants biochemically or using cell-based assays—improving speed of functional validation. In the era of WGS, noncoding variants are increasingly appearing, and their study necessitates a shift from the starting point of predictable amino acid consequence as can be determined in coding variants. <i>Hurabeille</i> et al. review how to determine the functional consequences of noncoding variants (i) utilizing natural genetic variation and CRISPR/Cas9 cellular engineering models, (ii) assessing chromatin accessibility, and (iii) applying multiplexed single-cell multiomic approaches.</p><p>The IEI landscape today is quite different from that in 1952…As Dorothy would say, <span><b><i>“Toto, I've a feeling we're not in Kansas anymore”.</i></b></span> Although the discovery and characterization of IEI have become more complex in the intervening decades, we summarize below how the reviews in this issue illustrate how IEI continue to illuminate mechanisms of human immunology (Figure 2).</p><p>The genetic theory of infectious disease formulated in the 1920s attempted to set the stage for a link between genes and immunity. But it was not until 1939, when Karl Diehl's and Otmar von Verschuer's studies of tuberculosis in monozygotic and dizygotic twins suggested that genetic factors contributed to tuberculosis susceptibility. Since then, several IEI underlying Mendelian Susceptibility of Mycobacterial Disease have been discovered;<span><sup>13</sup></span> along with many other monogenic defects that reveal specific mechanisms of antimicrobial immunity. Though the genetic determinants of antimicrobial immunity were not spotlighted until the 1950s, the function of human immune cells in combating infectious organisms were highlighted in the early 1900s. Nobel awards to Metchnikoff and Ehrlich in 1908 showcased the importance of phagocytosis in immunity. Metchnikoff even went on to postulate that intracellular digestion is important to maintain a balance between host intestinal immunity and microbiota—a founding principle of why phagocyte defects may present with (sometimes very early onset) inflammatory bowel disease (IBD), as discussed in <i>Zerbe</i> et al. (4) In their review, the authors describe different genetic <b><i>neutrophil defects</i></b> as paradigms of pathways critical to bacterial and antifungal immunity and IBD. While the infectious complications and antimicrobial prophylactic and/or treatment regimens for these IEI are similar, the underlying mechanisms of their autoinflammatory complications are distinct. Hence, a “precision medicine” approach to their inflammatory conditions requires the genetic diagnosis.</p><p>Neutrophil defects are not the only IEI that have enlightened <b><i>antifungal immunity</i></b>. <i>Vinh</i> (2) showed how the major molecular leap in understanding chronic mucocutaneous candidiasis (CMC) came with the genetic discovery of dominant-negative mutations in signal transducer and activator of transcription (STAT)3 in autosomal-dominant hyper-IgE syndrome (AD-HIES, also known as Job's syndrome).<span><sup>14, 15</sup></span> From this, it was deduced that defects in the T helper-producing interleukin (IL)-17 (Th17) subset of T cells, caused by the mutant STAT3, underlie CMC. Grounded on the principle of pathophysiologic homogeneity, this Th17 finding was a “pillar” that enabled the identification of numerous other IEI marked by CMC, converging on defective IL-17-based responses.<span><sup>16-21</sup></span> In their review, <i>Asano</i> et al. (5) focus on STAT1 gain-of-function (GOF), which accounts for approximately 50% of the genetic causality of CMC. STAT1 GOF patients show lower proportion of Th17 cells suggesting impaired differentiation.<span><sup>22</sup></span> Further support for the central role of the IL-17 axis in the immunopathogenesis of CMC is the correlation between this infection and the presence of neutralizing auto-antibodies (auto-Abs) to these mediators (IL-17A, IL-17, IL-22), as in autoimmune polyendocrinopathy-candidiasis-ectodermal dystrophy (APECED) or in CMC-affected thymoma patients,<span><sup>23, 24</sup></span> reviewed in <i>Vinh</i> (2) and <i>Bastard</i> et al (6). Moreover, production of such auto-Abs has been found to precede the infection, suggesting a causal role in the mycosis, rather than a consequence. Identifying the underlying etiology, whether it be a monogenic defect or a result of auto-Ab pathogenicity, determines distinct treatment paradigms, and once again highlights the importance of understanding the underlying immunogenetic mechanism in guiding precision medicine.</p><p>IEI patients with unique clinical infectious symptomatology have also enlightened mechanisms of <b><i>antiviral immunity</i></b>. <i>Gonench</i> et al. (7) review how viral infections may present with unusual manifestations with atypical or compensatory inflammatory responses. They particularly highlight how the vaccine strain of rubella virus can cause inflammatory granulomas in the skin and sometimes other tissues. The time between inoculation and pathogenic effects can be between three weeks and decades. Rates of virus-associated malignancies are also increased in patients with IEI. With these various complications, viral infections represent a significant source of morbidity in patients with IEI. Targeted cellular antiviral therapies borrowed from hematopoietic bone marrow transplant (HSCT) research are currently being applied to treat chronic viremia in IEI with specific viral susceptibility.<span><sup>25, 26</sup></span></p><p>The best-known case of IEI in popular culture is that of David Vetter (1971–1983), who had severe combined immunodeficiency (SCID) and lived in a sterile isolator for 12 years, known as the “bubble boy.” Since then, the <b><i>SCID diagnostic</i>, <i>genetic etiology</i>, <i>and treatment landscape</i></b> has dramatically changed as reviewed in <i>Aranda</i> et al. (8) Currently, 19 different genetic causes have been identified.<span><sup>2</sup></span> Yet, for some (~6–10%)<span><sup>27</sup></span> there is no known genetic basis. We can expect that this percentage will decrease yearly as additional IEI are discovered. For example, our group recently described how a hypomorphic LCK variant led to a SCID phenotype with autoinflammatory complications.<span><sup>28</sup></span> Newborn screening (NBS) has led to decreased morbidity and mortality, as patients are diagnosed soon after birth and HSCT can be pursued prior to occurrence of infectious complications. Furthermore, advances in gene therapy reviewed by <i>Kohn</i> et al. (9) and <i>Porteus</i> et al. (10) pave the road for precision medicine with curative goals for SCID.</p><p>As the number of causative genetic etiologies of SCID increased with NBS, so did our understanding of critical pathways in lymphocyte development, particularly T cells, as congenital athymia diagnoses also benefited from NBS. We and others describe how SCID NBS has helped reveal the true prevalence and socioeconomic burden of congenital athymia,<span><sup>29-31</sup></span> supporting the eventual FDA approval of thymic implantation. <i>Dinges</i> et al. (11) review <b><i>primary and secondary defects in the thymus</i></b>, which include natural aging and resultant thymic atrophy. The thymus is the primary site of T-cell development, enabling the generation and selection of a diverse T-cell repertoire that recognizes nonself, yet remains tolerant to self-antigens. Thymic output has been shown to be inversely correlated with the incidence of infections and cancer.<span><sup>32</sup></span> Hence, thymus defects lead to increased risk of infection, autoimmunity, and malignancy. Immunological outcomes of thymus removal in infancy (a byproduct of corrective surgery for congenital heart defects) and adulthood (i.e., thymoma, myasthenia gravis, etc.) have corroborated these findings. Thymectomized (young adult) patients demonstrate a decrease in naïve T-cell populations, T-cell oligoclonality, and increased expression of senescence markers—essentially T-cell phenotypes correlated with increased autoimmunity, malignancy, and mortality in the elderly.<span><sup>33, 34</sup></span></p><p>IEI associated with <b><i>thymic stromal defects</i></b> include those related to syndromes resulting from defective embryological processes that encompass structures of the midline, and specific genes critical to thymic development. For example, defects in forkhead box (FOX)N1, long appreciated as the cause of SCID in nude mice, have been recently identified as an IEI leading to congenital athymia in humans. FOXN1 is a member of the forkhead/winged helix family of transcription factors that controls the development, differentiation, and survival of skin epithelial cells and cortical and medullary thymic epithelial cells (mTECs) both during embryogenesis and in post-natal life. FOXN1 biallelic loss-of-function (LOF) and heterozygous LOF, demonstrate varying degrees of T-cell lymphopenia, infections, and autoimmunity, exemplifying the <i>one gene, different phenotypes</i> model and demonstrating the critical role of FOXN1 in different stages of T-cell development.<span><sup>35</sup></span> In their review, <i>Bastard</i> et al. (6) also show how different IEI affecting <b><i>central T</i>-<i>cell tolerance</i></b> illuminate the mechanism of <b><i>development of auto</i>-<i>Abs that neutralize type I interferon (IFN)</i></b>.<span><sup>36-38</sup></span> For example, more than 80% of patients with IEI in the alternative NF-kB pathway carry neutralizing auto-Abs to type I IFN.<span><sup>39</sup></span> In these patients, thymus structure is abnormal and expression of AIRE, a critical regulator of central T-cell tolerance, is impaired in mTECs. Auto-Ab neutralization of type I IFN persisted even after HSCT in these patients, further demonstrating that mTEC-intrinsic deficiency of AIRE underlies the development of auto-Abs against type I IFN, and ultimately predisposes patients to multiple viral infections.</p><p>In 1965, Bruce Glick and his colleagues wrote about their “suspicion regarding the importance of the bursa in antibody production.” Robert Good and Max Cooper revisited the role of the bursa and thymus in chickens and published an article in 1966 in the Journal of Experimental Medicine, where they showed that B (bursa-derived) cells are required for antibody responses, whereas T (thymus-derived) cells mediate delayed-type hypersensitivity reactions, such as graft-versus-host rejection.<span><sup>40</sup></span> Max Cooper, a pediatrician and clinical immunologist, went on to make a set of clinical observations about these two lineages. Boys with Wiskott–Aldrich syndrome developed widespread herpes viral lesions, yet had high levels of antibodies. In contrast, boys with agammaglobunemia could control viral infections even if they lacked antibody responses.<span><sup>41</sup></span></p><p><i>Tangye</i> et al. (12) review how IEI have illuminated <b><i>B</i>-<i>cell function and roles in immunological memory and host protection</i>, <i>as well as allergic disease</i></b>, through the lens of HIES due to STAT3 defects. <i>Tangye</i> et al. (12) take us on a journey that begins with the first demonstration, that germline heterozygous LOF/dominant negative (DN) mutations in STAT3 caused AD-HIES (2007), followed by the discovery of other genetic disorders in the IL-6 and IL-21 cytokine signaling pathways, which revealed the roles of each of these proteins in B-cell survival, isotype switching, and memory formation. For example, the function of ZNF341 has largely been elucidated by studies examining HIES patients, establishing its important role in regulating STAT3 expression and autoinduction.<span><sup>42-44</sup></span> <i>Tangye</i> et al. also discuss how studies of HIES have revealed aspects of (i) the interplay between STATs, (ii) the cytokines (and their signaling pathways) that are required for B-cell development and generation of long-lived humoral immunity and memory, and (iii) IL-6/STAT3 pathway defects and their role in dysregulated IgE production in IEI.</p><p>B-cell dysfunction in IEI has historically been associated with common variable immunodeficiency (CVID). <i>Romberg</i> et al. (13) review how <b><i>genetic variability</i>, <i>epigenetic changes</i>, <i>tolerogenic defects</i>, <i>and dysbiosis contribute to CVID heterogeneity</i></b>. The authors review the pathophysiology of CVID due to primary and secondary defects in B-cell activation, B-cell survival, regulatory T cell (Treg) dysfunction, B-cell tolerance, and aberrant germinal center (GC) dynamics. Their studies of malignancy-free excisional lymph node biopsies from CVID patients reveal that CVID GCs can either be diminutive or exuberantly hyperplastic and asymmetric. Correlation of these tissues with paired blood samples show that patients with hyperplastic GCs have the lowest serum IgA concentrations, the highest serum endotoxin concentrations, and invariably experience noninfectious complications, specifically autoimmune cytopenias. In contrast, patients manifesting only sinopulmonary infectious complications primarily display hypoplastic GCs. Our research group has also described peripheral blood immunological phenotypes involving T- and B-cell receptor signaling pathways, that best correlate with noninfectious outcomes in CVID, such as granulomatous lymphocytic interstitial lung disease.<span><sup>45</sup></span> Future validation of these findings may carry therapeutic ramifications for our ability to predict, which CVID patients will develop noninfectious complications.</p><p>This T–B cell interaction discussed in <i>Romberg</i> et al. (13) is also visited by <i>Borna</i> et al. (14) who review how Tregs may play a critical role in B-cell development including repertoire, and regulation of autoreactive (silenced) B cells in the periphery. Patients with IPEX have a transitional BCR repertoire that is similar to healthy individuals, whereas they have a mature naïve BCR repertoire that is enriched in autoreactive cells. Furthermore, autoreactive BCR repertoires are associated with other T-cell defects and silenced following gene therapy for T-cell defects. Taken together, these observations imply that Tregs may play a critical role in reducing numbers of autoreactive B cells in the periphery.</p><p>Patients characterized by noninfectious episodes of inflammation, but lacking high-titer autoantibodies or autoantigen-reactive T cells have violated the established dogma of autoreactivity.<span><sup>46, 47</sup></span> In the late 20th century, these disorders were termed <b><i>autoinflammatory syndromes</i></b> to distinguish them from autoimmune disorders. They were characterized molecularly by the identification of the genes whose defects caused four landmark hereditary periodic fever syndromes: TNF receptor super family member 1A (TNFRSF1A) in TNFR1-associated periodic syndromes (TRAPS), pyrin (MEFV) in familial Mediterranean fever, mevalonate kinase (MVK) in Hyper-IgD syndrome, and NLR pyrin domain containing 3 (NLRP3) in cryopyrin-associated autoinflammatory syndrome (CAPS). The group of contributing physician scientists in <i>Putnam</i> et al. (15) review NLRP3 inflammasome biology, a journey of discovery, which started from a case report in 1940 and led to the meeting of five families and 69 individuals with a lifelong history of cold-induced rash, fever, and arthralgias. The NLRP3 gene was cloned in 2001, followed by unraveling inflammasome biology including intracellular stress that triggers NLRP3 activation, genotype/phenotype associations in monogenic disease, protein structural analyses, mouse models of disease, and reaching their goal of targeted therapy with monoclonal antibodies that block IL-1 and IL-18, instigators of the patients' symptomatology.</p><p>Pathogenic variants perturbing proteasome molecules collectively known as <b><i>Proteasome associated autoinflammatory syndromes</i> (<i>PRAAS</i>)</b> result in proteasome deficiency and subsequent accumulation of ubiquitinated proteins. This pathologic build-up of proteins leads to unfolded protein response (UPR) that causes the expression of type I IFN genes. Hence, PRAAS are often considered a subclass of type I interferonopathy. <i>Poli</i> (16) reviews different IEI that underlie PRAAS, and the central role of proteasomes in cellular apoptotic function and immune response. Not surprisingly, defects in proteasomes lead to an increased IFN signature, and have been linked to autoimmune disease (such as lupus, myositis, or Sjogren syndrome) thereby exemplifying how molecular understanding of rare diseases exposes shared mechanisms with more common disorders. This <b>“<i>rare</i>-<i>to</i>-<i>common</i>” <i>paradigm</i></b> is also illustrated in <b><i>Down syndrome</i> (<i>DS</i>)</b> whereby insights from type I interferonopathies can be applied to our understanding of immunological implications of the most common genetic disorder associated with intellectual disability. <i>Ramba</i> et al. (17) review the clinical manifestations of increased infections and autoimmunity in DS, and how they are explained by specific immune cellular phenotypic and/or functional abnormalities. These abnormalities stem from increased type I and II IFN signaling due to increased IFN receptor expression (four out of six of the IFN receptor genes reside on chromosome 21). Along with the Espinosa lab, we have described in detail the downstream cellular effects of this increased interferon signature, along with multiple immunological and extra immunological manifestations associated with such cellular abnormalities.<span><sup>48, 49</sup></span> In fact, these clinical immunological and nonimmunological phenotypes of individuals with DS overlap with those of patients with STAT1 GOF or STAT3 GOF, implicating this pathway in a wide array of DS manifestations.<span><sup>50, 51</sup></span></p><p>Indeed, <i>Asano</i> et al. (5) review how <b><i>STAT1 GOF</i></b> results in the overproduction of IFN-α/β, IFN-γ, and IL-27, leading to immunodeficiency, autoimmunity, and/or cerebral aneurysm, among other complications. In contrast, Largent et al. recently demonstrated that it is the dysregulation of IFN-γ signaling in STAT1 GOF that promotes phenotypes associated with autoimmunity. They showed that STAT1 GOF autoimmunity is characterized by adaptive immune activation due to the dysregulation of STAT1 signaling through both type I and type II IFN receptors. Furthermore, they found that Stat1 GOF mice without type I IFN receptors were partially protected from STAT1-driven systemic inflammation, whereas the depletion of type II IFN receptors abrogated autoimmune manifestations. These results offer an intriguing new perspective on the relationship between IFN and STAT1 GOF, suggesting that activation via the IFN-γ receptor, rather than type I IFN, is essential for STAT1-dependent immune tolerance failure. This same concept is reviewed by <i>Chaimowitz</i> et al. (18) who extend the review to other JAK/STAT defects, their negative regulators' defects, and their causative roles in immune dysregulation, along with treatment choices in these disorders. Defects in JAK/STAT signaling provide another example of <i>one gene, multiple phenotypes</i>. IEI of STAT1 can be classified in four types of disease: autosomal recessive (AR) complete LOF, AR partial LOF, AD LOF, and AD GOF.<span><sup>52-56</sup></span> <i>Chaimowitz</i> et al. (18) review the body of literature describing the use of JAK inhibition in IEI resulting in JAK/STAT GOF phenotypes, type I interferonopathy, and PRAAS.</p><p>Monogenic disorders that impact Treg cell function or survival, are collectively called <b><i><b>Tregopathies</b></i></b>. <i>Borna</i> et al. (14) review the first Tregopathy disorder discovered, FOXP3 deficiency or IPEX. IPEX patients may present with normal T-cell count to low numbers of Tregs. In IPEX, the conventional memory T cells are usually increased as compared to the naïve subset and are skewed toward Th2 and/or Th17 over Th1 phenotype. <i>Borna</i> et al. (14) review how these T-cell subsets drive organ-specific autoimmunity, and how comparison of methylation and phenotypes suggests that Tregs in patients with IPEX may be somewhat plastic, becoming inflammatory T cells. Hence, pharmacological, or cellular therapeutic approaches to improve Treg numbers or function constitute a prime example of precision medicine in IEI. Not surprisingly, as the number of novel IEI recognized has increased, so have the genetic etiologies underlying Tregopathies, including IL-2Rβ defects described by our and the Lenardo groups in 2019.<span><sup>57-60</sup></span> Common presentations of these disorders include very early onset (VEO)-IBD, as reviewed by <i>Hall</i> et al. (19) To date, 80 monogenic causes of VEO-IBD have been identified and published. <i>Hall</i> et al. (19) review the different immunological pathways described in VEO-IBD and the burgeoning personalized therapy developing in this area.</p><p>Dr. Ogden not only described the first IEI, but he set the foundation for the first glimpse at precision medicine—the life-saving innovation of gamma globulin replacement therapy that has added decades to the lives of patients with humoral immune deficiencies. Since then, new generations of antimicrobials used prophylactically and/or therapeutically have reduced life-threatening fungal, bacterial, and viral infections in IEI. Autoimmune/inflammatory complications of IEI have historically been managed with nonspecific immunosuppression, such as glucocorticoids, cyclosporine, mycophenolate mofetil, etc. Advancements in the understanding of immune mechanisms of rheumatologic diseases led to the development and application of novel targeted therapeutics, including small molecule inhibitors, fusion proteins, and other biologics. These were <b><i>then</i> “<i>borrowed</i>” <i>and used for the treatment of IEI that involve aspects of autoimmunity</i>, <i>lymphoproliferation</i>, <i>and malignancy</i></b>.</p><p>For example, JAK inhibitors (JAKinibs) have proven effective in the treatment of rheumatoid arthritis (RA) and other immune mediated diseases,<span><sup>61</sup></span> and this paved the way for their use to treat immune dysregulation in patients with STAT1 and STAT3 GOF, as reviewed by <i>Chaimowitz</i> et al. (18) and <i>Asano</i> et al. (5) JAKinibs have also been used in type I interferonopathies as reviewed by <i>Ramba</i> et al. (17) and <i>Poli</i> (16). <i>Chaimowitz</i> et al. (18) review how tocilizumab, a humanized anti-IL-6 receptor monoclonal antibody that binds to soluble and membrane bound IL-6 receptors, has shown promise in the treatment of RA, and most recently STAT3 GOF. <i>Putnam</i> et al. (15) review how IL-1 blockade used in RA and systemic juvenile idiopathic arthritis (sJIA) have been used to treat CAPS. Abatacept, a soluble protein comprised of the extracellular domain of CTLA-4 linked to the Fc portion of IgG1 used in RA,<span><sup>62</sup></span> was also “borrowed” for use in CTLA-4 haploinsufficiency and LRBA deficiency.<span><sup>63-65</sup></span> In contrast, ipilimumab, an anti-CTLA-4 monoclonal antibody used to treat advanced stage melanoma, can “iatrogenically induce” the clinical autoimmune symptomatology of patients with CTLA-4 haploinsufficiency. We have published on the inverse correlation between the CTLA4 mRNA levels and degree of CTLA-4 pathway disruption, regardless of the etiology (genetic or iatrogenic).<span><sup>66</sup></span> Taken together, the mechanism of action of abatacept, ipilimumab, and the immunopathology of patients with CTLA-4 haploinsufficiency, reveal the relationship between rare diseases and common pathways in autoimmunity and malignancy.</p><p>Some of the challenges surrounding novel therapeutics specifically designed and approved for IEI are exacerbated by the rarity of these disorders, but we are beginning to see a “turning of the tide.” <i>Jordan</i> (20) reviews the pathophysiology, genetic etiologies, and targeted therapy development for patients with hemophagocytic lymphohistiocytosis (HLH) specifically. HLH is best conceptualized as a maladaptive state of excessive T-cell activation driving life-threatening myeloid cell activation, largely via IFNγ. The discovery of the key role of IFNγ in HLH pathogenesis in multiple murine models of HLH by independent laboratories spurred the clinical development of the neutralizing anti-IFNγ monoclonal antibody called emapalumab for use in patients with HLH. This development occurred relatively rapidly, taking only 14 years from initial publication of the therapeutic target to FDA approval of a clinical drug in 2020. Development and application of this therapy was unique in involving a number of firsts: the first trial of rationally targeted therapy in HLH, the first trial conducted per good clinical practice standards (or with industry sponsorship) in this disease entity, and the first drug ever approved by a regulatory agency for patients with HLH.</p><p>The use of these agents for the treatment of common autoimmune disorders exemplified the reduced scope of side effects, one of the main goals of precision medicine. But the “borrowed” indication of these agents to treat rare IEI best illustrated the concept of targeting the specific molecular basis of an immunologic disorder. JAKinibs inhibit the excessive activation of the JAK/STAT pathway in patients with STAT1/3 GOF, abatacept provides CTLA-4 to patients with CTLA-4 and LRBA deficiency who lack this T-cell activation inhibitory protein, IL-1 blockade neutralizes the downstream effects of the pro-inflammatory cytokines that patients with CAPS produce in excess. <b><i>These represent</i>, “<i>the right treatment for the right patient</i>.”</b> <i>But what about the</i> “<i>right time</i>?” Arguably, the “right time” to implement a treatment is to prevent end-organ damage effects, which is challenging in IEI given the common delay in diagnosis. In the advent of NBS for SCID, curative therapy via HSCT can now be implemented prior to development of life-threatening infections. And while HSCT is not exactly precise, it is still first line curative therapy in IEI until restoration of normal gene function via <b><i>gene therapy</i></b> approaches reach “prime time.” There have been both scientific and regulatory challenges along this road as highlighted by <i>Kohn</i> (9) and <i>Ghanim</i> et al. (10).</p><p>Traditionally, gene therapy approaches for IEI were attempted through gene addition using <b><i>retroviral or lentiviral vectors</i></b>. Although this has the advantage of sustained gene expression without requiring specific targeting by the vector, disadvantages, including lack of precise control over copy numbers and risk of random integration with possibility of leukemogenesis, placed gene therapy for X-linked SCID and CGD on hold for many years.<span><sup>67</sup></span> Early experience in gene therapy for adenosine deaminase (ADA) highlighted the critical importance of reconstituted cells having a selective advantage in success of the therapy—which sets the foundation for the higher success rate of HSCT for LOF disorders vs. GOF. With the shift of technology to lentiviral vector use, improvements in (i) cell culture and transduction efficiency cells, (ii) control over vector integration, and (iii) vector cryopreservation have made gene therapy more feasible for a greater number of patients, with a growing number of treated ADA patients demonstrating long term immune reconstitution. Gene therapy for ADA SCID has been approved by European regulators, however, the challenge of making definitive therapies for rare diseases commercially viable remains a major obstacle in reaching this goal.</p><p>Given the known serious complications in treating some IEI with gene addition approaches and advances in gene editing with <b><i>CRISPR</i>-<i>Cas9 technology</i></b>, many therapies are now focused on <b><i>correcting endogenous genes</i></b> as reviewed by <i>Ghanim</i> et al. (10) The major advantage of this approach is that endogenous regulation of gene expression is preserved—allowing normal expression during immune cell development and function. <i>Ghanim</i> et al. (10) illustrate the advantages of gene correction in several IEI, including B-cell tyrosine kinase (<i>BTK</i>), <i>CYBB, and FOXP3</i>. The challenge with gene editing approaches for personalized medicine will be in adapting approaches to ensure that they will benefit more than individual patients, or in achieving a new regulatory framework that is more permissive of personalized adaptation of therapies. Although gene therapy typically targets hematopoietic stem cells for a lasting cure, <i><b>targeting the pathologic cells is an alternative strategy</b>. Ghanim</i> et al (10). and <i>Borna</i> et al. (14), review one such strategy for replacing Tregs in IPEX. Autologous effector T cells can be transduced by a lentiviral vector expressing wild type FOXP3, which effectively transforms the cells to Tregs. This therapeutic approach is currently undergoing clinical trial. As cellular therapies continue to develop in oncology such the use of chimeric antigen receptor (CAR) T cells for lymphoma, and virus-specific T cells in HSCT, they will likely also be “borrowed” for treatment of IEI, and hopefully further illuminate mechanisms of pathway specific therapy.</p><p>What have IEI illuminated in human immunology since 1952? IEI are not as rare as we thought, but as a field we still need to undertake large collaborative efforts to follow the yellow brick road and reach the Emerald city. There is as much strength in publications from large numbers of patients from a multidisciplinary group, as there is from single patient case reports/research articles—a single grain of rice can tip the balance in our favor. While the toolbox to decipher novel IEI and dissect the causative molecular underpinnings of antimicrobial immunity and self-tolerance has expanded, so has the diversity of “flavors” of genetic etiologies in IEI. Encountering a variant in a known disease-related gene is not synonymous with pathogenicity. While experimental validation with either traditional immunological assays or high throughput variant functionalization approaches are still the gold standard to prove causation, they are labor intensive, often equating to a graduate student thesis and/or postdoctoral fellowship project, and hence not on clinically actionable timeline. Collaboration and sharing of data are still the most effective way to advance our understanding of human immunology, and importantly, help our patients.</p><p>Data sharing supports the ability to develop and apply machine learning methods, and thereby predict functional consequences. Perhaps, ChatGPT will replace researchers in IEI one day, but that day is not today. The advances in commercial machine learning that are reducing the costs of statistical prediction are simultaneously increasing the value of data (which enable prediction) and judgment (which determines why prediction matters). However, in IEI, when a patient does not “fit” the clinical picture typically seen for a given genetic disorder, instead of “judging the fit” we inquire “why does it not fit?” As long as we remain curious, and not judgmental, we academic physician-scientists stand a chance of keeping our jobs and not becoming an endangered species.</p><p>While we focus on gathering the data along the yellow brick road to the Emerald City of precise supportive and curative approaches in IEI (Figure 1), we must worry about the other “green” along the way; the for-profit biologic and cellular/gene therapy market is not always accessible to our “ultra-rare” patients. As we raise awareness of IEI across medical specialties outside of clinical immunology, we will likely gain visibility across pharmaceutical industry, NIH agencies, and FDA governance. Following the <i><b>yellow brick road</b></i> is not without challenges, but, just like Dorothy, we hopefully bring our <i><b>brains (scarecrow), heart (tinman), and courage (lion)</b></i> to help along the way.</p><p>This work was supported by the Jeffrey Modell Foundation Primary Immunodeficiency Center at Children's Hospital Colorado.</p><p>The author has no conflicts of interest to declare.</p>\",\"PeriodicalId\":178,\"journal\":{\"name\":\"Immunological Reviews\",\"volume\":\"322 1\",\"pages\":\"5-14\"},\"PeriodicalIF\":8.3000,\"publicationDate\":\"2024-02-02\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://onlinelibrary.wiley.com/doi/epdf/10.1111/imr.13311\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Immunological Reviews\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://onlinelibrary.wiley.com/doi/10.1111/imr.13311\",\"RegionNum\":2,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q1\",\"JCRName\":\"IMMUNOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Immunological Reviews","FirstCategoryId":"3","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1111/imr.13311","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"IMMUNOLOGY","Score":null,"Total":0}
Inborn errors of immunity illuminate mechanisms of human immunology and pave the road to precision medicine
The Yellow Brick Road leads Dorothy through Oz to the Emerald City—a luminescent green metropolis where she hopes to meet the great and powerful Wizard. The Emerald City is the destination of Dorothy's journey, where desires become reality. Arguably, the “Emerald City” for most physician-scientists caring for patients with inborn errors of immunity (IEI) is to apply effective therapies that target the specific impaired cell type/pathway, while avoiding detrimental effects on the rest of the immune system and other tissues (Figure 1). That is, to use the right treatment, at the right time, for the right patient—precision medicine at its best. The journey to this Emerald City has always started with the patient's symptoms and history. However, the constellation of these clinical clues has significantly changed over time, making it more challenging to begin the odyssey down the yellow brick road. In 1952, Dr. Ogden Bruton started his journey with patients who had recurrent pneumonias. Along the road, he found that they lacked serum γ-globulins. He then discovered a causative single gene defect, inherited as a Mendelian trait with full penetrance. Finally, he arrived at the targeted destination of immunoglobulin replacement therapy.1 Today, neither the starting point nor the road that follows are as straight and smooth.
As Bucciol et al. (1) describe in this issue, the wide availability and application of next-generation sequencing (NGS) methods, particularly whole exome/genome sequencing (WES/WGS), has significantly increased “the discovery rate” of additional IEI. The most recent International Union of Immunological Societies update (2022) included 55 novel monogenic gene defects, and one phenocopy due to autoantibodies discovered since January 2020, bringing the total number of IEI to 485.2 In some cases, distinct pathogenic variants at the same locus cause different IEI phenotypes (allelic heterogeneity; one gene, many phenotypes). In other cases, pathogenic variants in different genes governing one common pathway cause the same IEI (locus heterogeneity; many genes, one phenotype).3 Furthermore, as Vinh (2) discusses, IEI can also exemplify non-Mendelian basis of disease. While the overwhelming majority of IEI have been identified and mechanistically deciphered as monogenic, there are increasing reports of oligogenic IEI syndromes,4-8 wherein lesions in two or more distinct genes contribute to a clinical phenotype that has some features of the corresponding monogenic IEI disorders. Somatic mosaic mutations may lead to a milder or a more severe form of the disease, which may be influenced by the known pathogenicity of the mutation at the germline level.9 Alterations in gene expression such as DNA methylation and epigenetic modifications can also result in IEI. These new IEI expand beyond traditional boundaries, as recurrent infections are neither the only nor the most common clinical presentation. Clinical phenotypes as diverse as autoimmunity/inflammation, lymphoproliferation, malignancy, and severe allergy, involving multiple organs,10 have certainly expanded the breadth of IEI across medical and scientific fields. Consequently, the field of IEI has now adopted a “flying monkey's perspective” that now includes clinical subspecialties, where genetic etiology is not traditionally a cornerstone of the diagnostic work up. As we, clinical immunologists, strive to collaborate with other subspecialists to advocate for the importance of genetic testing and help with the interpretation of results, challenges surrounding cost and accessibility may deter genetic evaluation. We and others have published genetic testing recommendation guidelines11 to support the diagnostic odyssey and reduce delays in treatment.
Now, with great power comes great responsibility—while use of WES/WGS has led to the discovery of many new IEI and confers the power to “quickly” diagnose rare disease (completed in a clinical lab in days to weeks), it also often reveals the much-dreaded list of variants of unknown significance or VUS. Raising the questions—Who should establish if a VUS impairs a specific immune process and identify the associated phenotype, a.k.a functional validation? Who should fund this work? How long will it take? And do we wait until we have proven causality to determine a treatment course? The answer is it depends. When VUS are found in genes known to be associated with IEI, validation may involve evaluating protein expression or more complex cellular functional analyses (via clinical studies or research protocols). For VUS in genes not previously associated with IEI, first there is a “triage” process to decide whether further work up should be pursued. Once “triaged,” functional validation of these VUS typically requires lengthy and labor-intensive research evaluations necessary to prove causality—which are not compatible with “real time” clinical decision making. Hence, novel technologies are required to improve the “triage” and evaluation processes—making a case for deep immune profiling.12Hurabeille et al. (3) review emerging genomic tools to functionally assess candidate genetic variants. Functional genomics aims to understand the relationship between an organism's genome and its phenotype, which often display a hierarchical nature from molecular to organ-specific manifestations. High-throughput approaches to produce genetic variants, either with synthetic DNA sequences or direct endogenous genome editing has opened exciting avenues to study coding variants biochemically or using cell-based assays—improving speed of functional validation. In the era of WGS, noncoding variants are increasingly appearing, and their study necessitates a shift from the starting point of predictable amino acid consequence as can be determined in coding variants. Hurabeille et al. review how to determine the functional consequences of noncoding variants (i) utilizing natural genetic variation and CRISPR/Cas9 cellular engineering models, (ii) assessing chromatin accessibility, and (iii) applying multiplexed single-cell multiomic approaches.
The IEI landscape today is quite different from that in 1952…As Dorothy would say, “Toto, I've a feeling we're not in Kansas anymore”. Although the discovery and characterization of IEI have become more complex in the intervening decades, we summarize below how the reviews in this issue illustrate how IEI continue to illuminate mechanisms of human immunology (Figure 2).
The genetic theory of infectious disease formulated in the 1920s attempted to set the stage for a link between genes and immunity. But it was not until 1939, when Karl Diehl's and Otmar von Verschuer's studies of tuberculosis in monozygotic and dizygotic twins suggested that genetic factors contributed to tuberculosis susceptibility. Since then, several IEI underlying Mendelian Susceptibility of Mycobacterial Disease have been discovered;13 along with many other monogenic defects that reveal specific mechanisms of antimicrobial immunity. Though the genetic determinants of antimicrobial immunity were not spotlighted until the 1950s, the function of human immune cells in combating infectious organisms were highlighted in the early 1900s. Nobel awards to Metchnikoff and Ehrlich in 1908 showcased the importance of phagocytosis in immunity. Metchnikoff even went on to postulate that intracellular digestion is important to maintain a balance between host intestinal immunity and microbiota—a founding principle of why phagocyte defects may present with (sometimes very early onset) inflammatory bowel disease (IBD), as discussed in Zerbe et al. (4) In their review, the authors describe different genetic neutrophil defects as paradigms of pathways critical to bacterial and antifungal immunity and IBD. While the infectious complications and antimicrobial prophylactic and/or treatment regimens for these IEI are similar, the underlying mechanisms of their autoinflammatory complications are distinct. Hence, a “precision medicine” approach to their inflammatory conditions requires the genetic diagnosis.
Neutrophil defects are not the only IEI that have enlightened antifungal immunity. Vinh (2) showed how the major molecular leap in understanding chronic mucocutaneous candidiasis (CMC) came with the genetic discovery of dominant-negative mutations in signal transducer and activator of transcription (STAT)3 in autosomal-dominant hyper-IgE syndrome (AD-HIES, also known as Job's syndrome).14, 15 From this, it was deduced that defects in the T helper-producing interleukin (IL)-17 (Th17) subset of T cells, caused by the mutant STAT3, underlie CMC. Grounded on the principle of pathophysiologic homogeneity, this Th17 finding was a “pillar” that enabled the identification of numerous other IEI marked by CMC, converging on defective IL-17-based responses.16-21 In their review, Asano et al. (5) focus on STAT1 gain-of-function (GOF), which accounts for approximately 50% of the genetic causality of CMC. STAT1 GOF patients show lower proportion of Th17 cells suggesting impaired differentiation.22 Further support for the central role of the IL-17 axis in the immunopathogenesis of CMC is the correlation between this infection and the presence of neutralizing auto-antibodies (auto-Abs) to these mediators (IL-17A, IL-17, IL-22), as in autoimmune polyendocrinopathy-candidiasis-ectodermal dystrophy (APECED) or in CMC-affected thymoma patients,23, 24 reviewed in Vinh (2) and Bastard et al (6). Moreover, production of such auto-Abs has been found to precede the infection, suggesting a causal role in the mycosis, rather than a consequence. Identifying the underlying etiology, whether it be a monogenic defect or a result of auto-Ab pathogenicity, determines distinct treatment paradigms, and once again highlights the importance of understanding the underlying immunogenetic mechanism in guiding precision medicine.
IEI patients with unique clinical infectious symptomatology have also enlightened mechanisms of antiviral immunity. Gonench et al. (7) review how viral infections may present with unusual manifestations with atypical or compensatory inflammatory responses. They particularly highlight how the vaccine strain of rubella virus can cause inflammatory granulomas in the skin and sometimes other tissues. The time between inoculation and pathogenic effects can be between three weeks and decades. Rates of virus-associated malignancies are also increased in patients with IEI. With these various complications, viral infections represent a significant source of morbidity in patients with IEI. Targeted cellular antiviral therapies borrowed from hematopoietic bone marrow transplant (HSCT) research are currently being applied to treat chronic viremia in IEI with specific viral susceptibility.25, 26
The best-known case of IEI in popular culture is that of David Vetter (1971–1983), who had severe combined immunodeficiency (SCID) and lived in a sterile isolator for 12 years, known as the “bubble boy.” Since then, the SCID diagnostic, genetic etiology, and treatment landscape has dramatically changed as reviewed in Aranda et al. (8) Currently, 19 different genetic causes have been identified.2 Yet, for some (~6–10%)27 there is no known genetic basis. We can expect that this percentage will decrease yearly as additional IEI are discovered. For example, our group recently described how a hypomorphic LCK variant led to a SCID phenotype with autoinflammatory complications.28 Newborn screening (NBS) has led to decreased morbidity and mortality, as patients are diagnosed soon after birth and HSCT can be pursued prior to occurrence of infectious complications. Furthermore, advances in gene therapy reviewed by Kohn et al. (9) and Porteus et al. (10) pave the road for precision medicine with curative goals for SCID.
As the number of causative genetic etiologies of SCID increased with NBS, so did our understanding of critical pathways in lymphocyte development, particularly T cells, as congenital athymia diagnoses also benefited from NBS. We and others describe how SCID NBS has helped reveal the true prevalence and socioeconomic burden of congenital athymia,29-31 supporting the eventual FDA approval of thymic implantation. Dinges et al. (11) review primary and secondary defects in the thymus, which include natural aging and resultant thymic atrophy. The thymus is the primary site of T-cell development, enabling the generation and selection of a diverse T-cell repertoire that recognizes nonself, yet remains tolerant to self-antigens. Thymic output has been shown to be inversely correlated with the incidence of infections and cancer.32 Hence, thymus defects lead to increased risk of infection, autoimmunity, and malignancy. Immunological outcomes of thymus removal in infancy (a byproduct of corrective surgery for congenital heart defects) and adulthood (i.e., thymoma, myasthenia gravis, etc.) have corroborated these findings. Thymectomized (young adult) patients demonstrate a decrease in naïve T-cell populations, T-cell oligoclonality, and increased expression of senescence markers—essentially T-cell phenotypes correlated with increased autoimmunity, malignancy, and mortality in the elderly.33, 34
IEI associated with thymic stromal defects include those related to syndromes resulting from defective embryological processes that encompass structures of the midline, and specific genes critical to thymic development. For example, defects in forkhead box (FOX)N1, long appreciated as the cause of SCID in nude mice, have been recently identified as an IEI leading to congenital athymia in humans. FOXN1 is a member of the forkhead/winged helix family of transcription factors that controls the development, differentiation, and survival of skin epithelial cells and cortical and medullary thymic epithelial cells (mTECs) both during embryogenesis and in post-natal life. FOXN1 biallelic loss-of-function (LOF) and heterozygous LOF, demonstrate varying degrees of T-cell lymphopenia, infections, and autoimmunity, exemplifying the one gene, different phenotypes model and demonstrating the critical role of FOXN1 in different stages of T-cell development.35 In their review, Bastard et al. (6) also show how different IEI affecting central T-cell tolerance illuminate the mechanism of development of auto-Abs that neutralize type I interferon (IFN).36-38 For example, more than 80% of patients with IEI in the alternative NF-kB pathway carry neutralizing auto-Abs to type I IFN.39 In these patients, thymus structure is abnormal and expression of AIRE, a critical regulator of central T-cell tolerance, is impaired in mTECs. Auto-Ab neutralization of type I IFN persisted even after HSCT in these patients, further demonstrating that mTEC-intrinsic deficiency of AIRE underlies the development of auto-Abs against type I IFN, and ultimately predisposes patients to multiple viral infections.
In 1965, Bruce Glick and his colleagues wrote about their “suspicion regarding the importance of the bursa in antibody production.” Robert Good and Max Cooper revisited the role of the bursa and thymus in chickens and published an article in 1966 in the Journal of Experimental Medicine, where they showed that B (bursa-derived) cells are required for antibody responses, whereas T (thymus-derived) cells mediate delayed-type hypersensitivity reactions, such as graft-versus-host rejection.40 Max Cooper, a pediatrician and clinical immunologist, went on to make a set of clinical observations about these two lineages. Boys with Wiskott–Aldrich syndrome developed widespread herpes viral lesions, yet had high levels of antibodies. In contrast, boys with agammaglobunemia could control viral infections even if they lacked antibody responses.41
Tangye et al. (12) review how IEI have illuminated B-cell function and roles in immunological memory and host protection, as well as allergic disease, through the lens of HIES due to STAT3 defects. Tangye et al. (12) take us on a journey that begins with the first demonstration, that germline heterozygous LOF/dominant negative (DN) mutations in STAT3 caused AD-HIES (2007), followed by the discovery of other genetic disorders in the IL-6 and IL-21 cytokine signaling pathways, which revealed the roles of each of these proteins in B-cell survival, isotype switching, and memory formation. For example, the function of ZNF341 has largely been elucidated by studies examining HIES patients, establishing its important role in regulating STAT3 expression and autoinduction.42-44Tangye et al. also discuss how studies of HIES have revealed aspects of (i) the interplay between STATs, (ii) the cytokines (and their signaling pathways) that are required for B-cell development and generation of long-lived humoral immunity and memory, and (iii) IL-6/STAT3 pathway defects and their role in dysregulated IgE production in IEI.
B-cell dysfunction in IEI has historically been associated with common variable immunodeficiency (CVID). Romberg et al. (13) review how genetic variability, epigenetic changes, tolerogenic defects, and dysbiosis contribute to CVID heterogeneity. The authors review the pathophysiology of CVID due to primary and secondary defects in B-cell activation, B-cell survival, regulatory T cell (Treg) dysfunction, B-cell tolerance, and aberrant germinal center (GC) dynamics. Their studies of malignancy-free excisional lymph node biopsies from CVID patients reveal that CVID GCs can either be diminutive or exuberantly hyperplastic and asymmetric. Correlation of these tissues with paired blood samples show that patients with hyperplastic GCs have the lowest serum IgA concentrations, the highest serum endotoxin concentrations, and invariably experience noninfectious complications, specifically autoimmune cytopenias. In contrast, patients manifesting only sinopulmonary infectious complications primarily display hypoplastic GCs. Our research group has also described peripheral blood immunological phenotypes involving T- and B-cell receptor signaling pathways, that best correlate with noninfectious outcomes in CVID, such as granulomatous lymphocytic interstitial lung disease.45 Future validation of these findings may carry therapeutic ramifications for our ability to predict, which CVID patients will develop noninfectious complications.
This T–B cell interaction discussed in Romberg et al. (13) is also visited by Borna et al. (14) who review how Tregs may play a critical role in B-cell development including repertoire, and regulation of autoreactive (silenced) B cells in the periphery. Patients with IPEX have a transitional BCR repertoire that is similar to healthy individuals, whereas they have a mature naïve BCR repertoire that is enriched in autoreactive cells. Furthermore, autoreactive BCR repertoires are associated with other T-cell defects and silenced following gene therapy for T-cell defects. Taken together, these observations imply that Tregs may play a critical role in reducing numbers of autoreactive B cells in the periphery.
Patients characterized by noninfectious episodes of inflammation, but lacking high-titer autoantibodies or autoantigen-reactive T cells have violated the established dogma of autoreactivity.46, 47 In the late 20th century, these disorders were termed autoinflammatory syndromes to distinguish them from autoimmune disorders. They were characterized molecularly by the identification of the genes whose defects caused four landmark hereditary periodic fever syndromes: TNF receptor super family member 1A (TNFRSF1A) in TNFR1-associated periodic syndromes (TRAPS), pyrin (MEFV) in familial Mediterranean fever, mevalonate kinase (MVK) in Hyper-IgD syndrome, and NLR pyrin domain containing 3 (NLRP3) in cryopyrin-associated autoinflammatory syndrome (CAPS). The group of contributing physician scientists in Putnam et al. (15) review NLRP3 inflammasome biology, a journey of discovery, which started from a case report in 1940 and led to the meeting of five families and 69 individuals with a lifelong history of cold-induced rash, fever, and arthralgias. The NLRP3 gene was cloned in 2001, followed by unraveling inflammasome biology including intracellular stress that triggers NLRP3 activation, genotype/phenotype associations in monogenic disease, protein structural analyses, mouse models of disease, and reaching their goal of targeted therapy with monoclonal antibodies that block IL-1 and IL-18, instigators of the patients' symptomatology.
Pathogenic variants perturbing proteasome molecules collectively known as Proteasome associated autoinflammatory syndromes (PRAAS) result in proteasome deficiency and subsequent accumulation of ubiquitinated proteins. This pathologic build-up of proteins leads to unfolded protein response (UPR) that causes the expression of type I IFN genes. Hence, PRAAS are often considered a subclass of type I interferonopathy. Poli (16) reviews different IEI that underlie PRAAS, and the central role of proteasomes in cellular apoptotic function and immune response. Not surprisingly, defects in proteasomes lead to an increased IFN signature, and have been linked to autoimmune disease (such as lupus, myositis, or Sjogren syndrome) thereby exemplifying how molecular understanding of rare diseases exposes shared mechanisms with more common disorders. This “rare-to-common” paradigm is also illustrated in Down syndrome (DS) whereby insights from type I interferonopathies can be applied to our understanding of immunological implications of the most common genetic disorder associated with intellectual disability. Ramba et al. (17) review the clinical manifestations of increased infections and autoimmunity in DS, and how they are explained by specific immune cellular phenotypic and/or functional abnormalities. These abnormalities stem from increased type I and II IFN signaling due to increased IFN receptor expression (four out of six of the IFN receptor genes reside on chromosome 21). Along with the Espinosa lab, we have described in detail the downstream cellular effects of this increased interferon signature, along with multiple immunological and extra immunological manifestations associated with such cellular abnormalities.48, 49 In fact, these clinical immunological and nonimmunological phenotypes of individuals with DS overlap with those of patients with STAT1 GOF or STAT3 GOF, implicating this pathway in a wide array of DS manifestations.50, 51
Indeed, Asano et al. (5) review how STAT1 GOF results in the overproduction of IFN-α/β, IFN-γ, and IL-27, leading to immunodeficiency, autoimmunity, and/or cerebral aneurysm, among other complications. In contrast, Largent et al. recently demonstrated that it is the dysregulation of IFN-γ signaling in STAT1 GOF that promotes phenotypes associated with autoimmunity. They showed that STAT1 GOF autoimmunity is characterized by adaptive immune activation due to the dysregulation of STAT1 signaling through both type I and type II IFN receptors. Furthermore, they found that Stat1 GOF mice without type I IFN receptors were partially protected from STAT1-driven systemic inflammation, whereas the depletion of type II IFN receptors abrogated autoimmune manifestations. These results offer an intriguing new perspective on the relationship between IFN and STAT1 GOF, suggesting that activation via the IFN-γ receptor, rather than type I IFN, is essential for STAT1-dependent immune tolerance failure. This same concept is reviewed by Chaimowitz et al. (18) who extend the review to other JAK/STAT defects, their negative regulators' defects, and their causative roles in immune dysregulation, along with treatment choices in these disorders. Defects in JAK/STAT signaling provide another example of one gene, multiple phenotypes. IEI of STAT1 can be classified in four types of disease: autosomal recessive (AR) complete LOF, AR partial LOF, AD LOF, and AD GOF.52-56Chaimowitz et al. (18) review the body of literature describing the use of JAK inhibition in IEI resulting in JAK/STAT GOF phenotypes, type I interferonopathy, and PRAAS.
Monogenic disorders that impact Treg cell function or survival, are collectively called Tregopathies. Borna et al. (14) review the first Tregopathy disorder discovered, FOXP3 deficiency or IPEX. IPEX patients may present with normal T-cell count to low numbers of Tregs. In IPEX, the conventional memory T cells are usually increased as compared to the naïve subset and are skewed toward Th2 and/or Th17 over Th1 phenotype. Borna et al. (14) review how these T-cell subsets drive organ-specific autoimmunity, and how comparison of methylation and phenotypes suggests that Tregs in patients with IPEX may be somewhat plastic, becoming inflammatory T cells. Hence, pharmacological, or cellular therapeutic approaches to improve Treg numbers or function constitute a prime example of precision medicine in IEI. Not surprisingly, as the number of novel IEI recognized has increased, so have the genetic etiologies underlying Tregopathies, including IL-2Rβ defects described by our and the Lenardo groups in 2019.57-60 Common presentations of these disorders include very early onset (VEO)-IBD, as reviewed by Hall et al. (19) To date, 80 monogenic causes of VEO-IBD have been identified and published. Hall et al. (19) review the different immunological pathways described in VEO-IBD and the burgeoning personalized therapy developing in this area.
Dr. Ogden not only described the first IEI, but he set the foundation for the first glimpse at precision medicine—the life-saving innovation of gamma globulin replacement therapy that has added decades to the lives of patients with humoral immune deficiencies. Since then, new generations of antimicrobials used prophylactically and/or therapeutically have reduced life-threatening fungal, bacterial, and viral infections in IEI. Autoimmune/inflammatory complications of IEI have historically been managed with nonspecific immunosuppression, such as glucocorticoids, cyclosporine, mycophenolate mofetil, etc. Advancements in the understanding of immune mechanisms of rheumatologic diseases led to the development and application of novel targeted therapeutics, including small molecule inhibitors, fusion proteins, and other biologics. These were then “borrowed” and used for the treatment of IEI that involve aspects of autoimmunity, lymphoproliferation, and malignancy.
For example, JAK inhibitors (JAKinibs) have proven effective in the treatment of rheumatoid arthritis (RA) and other immune mediated diseases,61 and this paved the way for their use to treat immune dysregulation in patients with STAT1 and STAT3 GOF, as reviewed by Chaimowitz et al. (18) and Asano et al. (5) JAKinibs have also been used in type I interferonopathies as reviewed by Ramba et al. (17) and Poli (16). Chaimowitz et al. (18) review how tocilizumab, a humanized anti-IL-6 receptor monoclonal antibody that binds to soluble and membrane bound IL-6 receptors, has shown promise in the treatment of RA, and most recently STAT3 GOF. Putnam et al. (15) review how IL-1 blockade used in RA and systemic juvenile idiopathic arthritis (sJIA) have been used to treat CAPS. Abatacept, a soluble protein comprised of the extracellular domain of CTLA-4 linked to the Fc portion of IgG1 used in RA,62 was also “borrowed” for use in CTLA-4 haploinsufficiency and LRBA deficiency.63-65 In contrast, ipilimumab, an anti-CTLA-4 monoclonal antibody used to treat advanced stage melanoma, can “iatrogenically induce” the clinical autoimmune symptomatology of patients with CTLA-4 haploinsufficiency. We have published on the inverse correlation between the CTLA4 mRNA levels and degree of CTLA-4 pathway disruption, regardless of the etiology (genetic or iatrogenic).66 Taken together, the mechanism of action of abatacept, ipilimumab, and the immunopathology of patients with CTLA-4 haploinsufficiency, reveal the relationship between rare diseases and common pathways in autoimmunity and malignancy.
Some of the challenges surrounding novel therapeutics specifically designed and approved for IEI are exacerbated by the rarity of these disorders, but we are beginning to see a “turning of the tide.” Jordan (20) reviews the pathophysiology, genetic etiologies, and targeted therapy development for patients with hemophagocytic lymphohistiocytosis (HLH) specifically. HLH is best conceptualized as a maladaptive state of excessive T-cell activation driving life-threatening myeloid cell activation, largely via IFNγ. The discovery of the key role of IFNγ in HLH pathogenesis in multiple murine models of HLH by independent laboratories spurred the clinical development of the neutralizing anti-IFNγ monoclonal antibody called emapalumab for use in patients with HLH. This development occurred relatively rapidly, taking only 14 years from initial publication of the therapeutic target to FDA approval of a clinical drug in 2020. Development and application of this therapy was unique in involving a number of firsts: the first trial of rationally targeted therapy in HLH, the first trial conducted per good clinical practice standards (or with industry sponsorship) in this disease entity, and the first drug ever approved by a regulatory agency for patients with HLH.
The use of these agents for the treatment of common autoimmune disorders exemplified the reduced scope of side effects, one of the main goals of precision medicine. But the “borrowed” indication of these agents to treat rare IEI best illustrated the concept of targeting the specific molecular basis of an immunologic disorder. JAKinibs inhibit the excessive activation of the JAK/STAT pathway in patients with STAT1/3 GOF, abatacept provides CTLA-4 to patients with CTLA-4 and LRBA deficiency who lack this T-cell activation inhibitory protein, IL-1 blockade neutralizes the downstream effects of the pro-inflammatory cytokines that patients with CAPS produce in excess. These represent, “the right treatment for the right patient.”But what about the “right time?” Arguably, the “right time” to implement a treatment is to prevent end-organ damage effects, which is challenging in IEI given the common delay in diagnosis. In the advent of NBS for SCID, curative therapy via HSCT can now be implemented prior to development of life-threatening infections. And while HSCT is not exactly precise, it is still first line curative therapy in IEI until restoration of normal gene function via gene therapy approaches reach “prime time.” There have been both scientific and regulatory challenges along this road as highlighted by Kohn (9) and Ghanim et al. (10).
Traditionally, gene therapy approaches for IEI were attempted through gene addition using retroviral or lentiviral vectors. Although this has the advantage of sustained gene expression without requiring specific targeting by the vector, disadvantages, including lack of precise control over copy numbers and risk of random integration with possibility of leukemogenesis, placed gene therapy for X-linked SCID and CGD on hold for many years.67 Early experience in gene therapy for adenosine deaminase (ADA) highlighted the critical importance of reconstituted cells having a selective advantage in success of the therapy—which sets the foundation for the higher success rate of HSCT for LOF disorders vs. GOF. With the shift of technology to lentiviral vector use, improvements in (i) cell culture and transduction efficiency cells, (ii) control over vector integration, and (iii) vector cryopreservation have made gene therapy more feasible for a greater number of patients, with a growing number of treated ADA patients demonstrating long term immune reconstitution. Gene therapy for ADA SCID has been approved by European regulators, however, the challenge of making definitive therapies for rare diseases commercially viable remains a major obstacle in reaching this goal.
Given the known serious complications in treating some IEI with gene addition approaches and advances in gene editing with CRISPR-Cas9 technology, many therapies are now focused on correcting endogenous genes as reviewed by Ghanim et al. (10) The major advantage of this approach is that endogenous regulation of gene expression is preserved—allowing normal expression during immune cell development and function. Ghanim et al. (10) illustrate the advantages of gene correction in several IEI, including B-cell tyrosine kinase (BTK), CYBB, and FOXP3. The challenge with gene editing approaches for personalized medicine will be in adapting approaches to ensure that they will benefit more than individual patients, or in achieving a new regulatory framework that is more permissive of personalized adaptation of therapies. Although gene therapy typically targets hematopoietic stem cells for a lasting cure, targeting the pathologic cells is an alternative strategy. Ghanim et al (10). and Borna et al. (14), review one such strategy for replacing Tregs in IPEX. Autologous effector T cells can be transduced by a lentiviral vector expressing wild type FOXP3, which effectively transforms the cells to Tregs. This therapeutic approach is currently undergoing clinical trial. As cellular therapies continue to develop in oncology such the use of chimeric antigen receptor (CAR) T cells for lymphoma, and virus-specific T cells in HSCT, they will likely also be “borrowed” for treatment of IEI, and hopefully further illuminate mechanisms of pathway specific therapy.
What have IEI illuminated in human immunology since 1952? IEI are not as rare as we thought, but as a field we still need to undertake large collaborative efforts to follow the yellow brick road and reach the Emerald city. There is as much strength in publications from large numbers of patients from a multidisciplinary group, as there is from single patient case reports/research articles—a single grain of rice can tip the balance in our favor. While the toolbox to decipher novel IEI and dissect the causative molecular underpinnings of antimicrobial immunity and self-tolerance has expanded, so has the diversity of “flavors” of genetic etiologies in IEI. Encountering a variant in a known disease-related gene is not synonymous with pathogenicity. While experimental validation with either traditional immunological assays or high throughput variant functionalization approaches are still the gold standard to prove causation, they are labor intensive, often equating to a graduate student thesis and/or postdoctoral fellowship project, and hence not on clinically actionable timeline. Collaboration and sharing of data are still the most effective way to advance our understanding of human immunology, and importantly, help our patients.
Data sharing supports the ability to develop and apply machine learning methods, and thereby predict functional consequences. Perhaps, ChatGPT will replace researchers in IEI one day, but that day is not today. The advances in commercial machine learning that are reducing the costs of statistical prediction are simultaneously increasing the value of data (which enable prediction) and judgment (which determines why prediction matters). However, in IEI, when a patient does not “fit” the clinical picture typically seen for a given genetic disorder, instead of “judging the fit” we inquire “why does it not fit?” As long as we remain curious, and not judgmental, we academic physician-scientists stand a chance of keeping our jobs and not becoming an endangered species.
While we focus on gathering the data along the yellow brick road to the Emerald City of precise supportive and curative approaches in IEI (Figure 1), we must worry about the other “green” along the way; the for-profit biologic and cellular/gene therapy market is not always accessible to our “ultra-rare” patients. As we raise awareness of IEI across medical specialties outside of clinical immunology, we will likely gain visibility across pharmaceutical industry, NIH agencies, and FDA governance. Following the yellow brick road is not without challenges, but, just like Dorothy, we hopefully bring our brains (scarecrow), heart (tinman), and courage (lion) to help along the way.
This work was supported by the Jeffrey Modell Foundation Primary Immunodeficiency Center at Children's Hospital Colorado.
The author has no conflicts of interest to declare.
期刊介绍:
Immunological Reviews is a specialized journal that focuses on various aspects of immunological research. It encompasses a wide range of topics, such as clinical immunology, experimental immunology, and investigations related to allergy and the immune system.
The journal follows a unique approach where each volume is dedicated solely to a specific area of immunological research. However, collectively, these volumes aim to offer an extensive and up-to-date overview of the latest advancements in basic immunology and their practical implications in clinical settings.
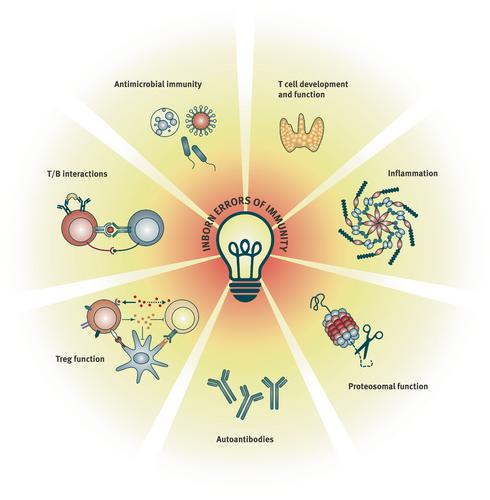



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
