Leevi A Toivonen, Heikki Mäntymäki, Lorin M Benneker, Hannu Kautiainen, Arja Häkkinen, Marko H Neva
{"title":"颅骨邻近椎间盘退变对腰椎融合术后 12 年累计翻修风险的非线性影响。","authors":"Leevi A Toivonen, Heikki Mäntymäki, Lorin M Benneker, Hannu Kautiainen, Arja Häkkinen, Marko H Neva","doi":"10.1097/BRS.0000000000004949","DOIUrl":null,"url":null,"abstract":"<p><strong>Study design: </strong>Retrospective analysis of prospectively collected data.</p><p><strong>Objective: </strong>To evaluate how preexisting adjacent segment degeneration status impacts revision risk for adjacent segment disease (ASD) after lumbar fusions.</p><p><strong>Summary of background data: </strong>ASD incurs late reoperations after lumbar fusion surgeries. ASD pathogenesis is multifactorial. Preexisting adjacent segment degeneration, measured by Pfirrmann, is suggested as one of the predisposing factors. We sought to find deeper insights into this association by using a more granular degeneration measure, the combined imaging score (CIS).</p><p><strong>Patients and methods: </strong>A total of 197 consecutive lumbar fusions for degenerative pathologies were enrolled in a prospective follow-up (median: 12 yr). Preoperative cranial adjacent segment degeneration status was determined using Pfirrmann and CIS, which utilize both radiographs and magnetic resonance imaging. On the basis of CIS, patients were trichotomized into tertiles (CIS <7, CIS 7-10, and CIS >10). The cumulative ASD revision risk was determined for each tertile. After adjusting for age, sex, body mass index, sacral fixation, and fusion length, hazard ratios (95% CI) for ASD revisions were determined for each Pfirrmann and CIS score.</p><p><strong>Results: </strong>Patients in the intermediate CIS tertile had a cumulative ASD revision risk of 25.4% (17.0%-37.0%), while both milder degeneration (CIS <7) [13.2% (6.5%-25.8%)] and end-stage degeneration (CIS >10) [13.6% (7.0%-25.5%)] appeared to be protective against surgical ASD. Pfirrmann failed to show a significant association with ASD revision risk. Adjusted analysis of CIS suggested increased ASD revisions after CIS 7, which turned contrariwise after CIS 10.</p><p><strong>Conclusions: </strong>The effect of preexisting adjacent segment degeneration on ASD reoperation risk is not linear. The risk appears to increase with advancing degeneration but diminishes with end-stage degeneration. Therefore, end-stage degenerative segments may be considered to be excluded from fusion constructs.</p><p><strong>Level of evidence: </strong>Therapeutic 3.</p>","PeriodicalId":22193,"journal":{"name":"Spine","volume":" ","pages":"E372-E377"},"PeriodicalIF":3.5000,"publicationDate":"2024-11-15","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11512618/pdf/","citationCount":"0","resultStr":"{\"title\":\"Nonlinear Effect of Preexisting Cranial Adjacent Disc Degeneration on Cumulative 12-Year Revision Risk Following Lumbar Fusions.\",\"authors\":\"Leevi A Toivonen, Heikki Mäntymäki, Lorin M Benneker, Hannu Kautiainen, Arja Häkkinen, Marko H Neva\",\"doi\":\"10.1097/BRS.0000000000004949\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Study design: </strong>Retrospective analysis of prospectively collected data.</p><p><strong>Objective: </strong>To evaluate how preexisting adjacent segment degeneration status impacts revision risk for adjacent segment disease (ASD) after lumbar fusions.</p><p><strong>Summary of background data: </strong>ASD incurs late reoperations after lumbar fusion surgeries. ASD pathogenesis is multifactorial. Preexisting adjacent segment degeneration, measured by Pfirrmann, is suggested as one of the predisposing factors. We sought to find deeper insights into this association by using a more granular degeneration measure, the combined imaging score (CIS).</p><p><strong>Patients and methods: </strong>A total of 197 consecutive lumbar fusions for degenerative pathologies were enrolled in a prospective follow-up (median: 12 yr). Preoperative cranial adjacent segment degeneration status was determined using Pfirrmann and CIS, which utilize both radiographs and magnetic resonance imaging. On the basis of CIS, patients were trichotomized into tertiles (CIS <7, CIS 7-10, and CIS >10). The cumulative ASD revision risk was determined for each tertile. After adjusting for age, sex, body mass index, sacral fixation, and fusion length, hazard ratios (95% CI) for ASD revisions were determined for each Pfirrmann and CIS score.</p><p><strong>Results: </strong>Patients in the intermediate CIS tertile had a cumulative ASD revision risk of 25.4% (17.0%-37.0%), while both milder degeneration (CIS <7) [13.2% (6.5%-25.8%)] and end-stage degeneration (CIS >10) [13.6% (7.0%-25.5%)] appeared to be protective against surgical ASD. Pfirrmann failed to show a significant association with ASD revision risk. Adjusted analysis of CIS suggested increased ASD revisions after CIS 7, which turned contrariwise after CIS 10.</p><p><strong>Conclusions: </strong>The effect of preexisting adjacent segment degeneration on ASD reoperation risk is not linear. The risk appears to increase with advancing degeneration but diminishes with end-stage degeneration. Therefore, end-stage degenerative segments may be considered to be excluded from fusion constructs.</p><p><strong>Level of evidence: </strong>Therapeutic 3.</p>\",\"PeriodicalId\":22193,\"journal\":{\"name\":\"Spine\",\"volume\":\" \",\"pages\":\"E372-E377\"},\"PeriodicalIF\":3.5000,\"publicationDate\":\"2024-11-15\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11512618/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Spine\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1097/BRS.0000000000004949\",\"RegionNum\":2,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2024/2/2 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q2\",\"JCRName\":\"CLINICAL NEUROLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Spine","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1097/BRS.0000000000004949","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/2/2 0:00:00","PubModel":"Epub","JCR":"Q2","JCRName":"CLINICAL NEUROLOGY","Score":null,"Total":0}
Nonlinear Effect of Preexisting Cranial Adjacent Disc Degeneration on Cumulative 12-Year Revision Risk Following Lumbar Fusions.
Study design: Retrospective analysis of prospectively collected data.
Objective: To evaluate how preexisting adjacent segment degeneration status impacts revision risk for adjacent segment disease (ASD) after lumbar fusions.
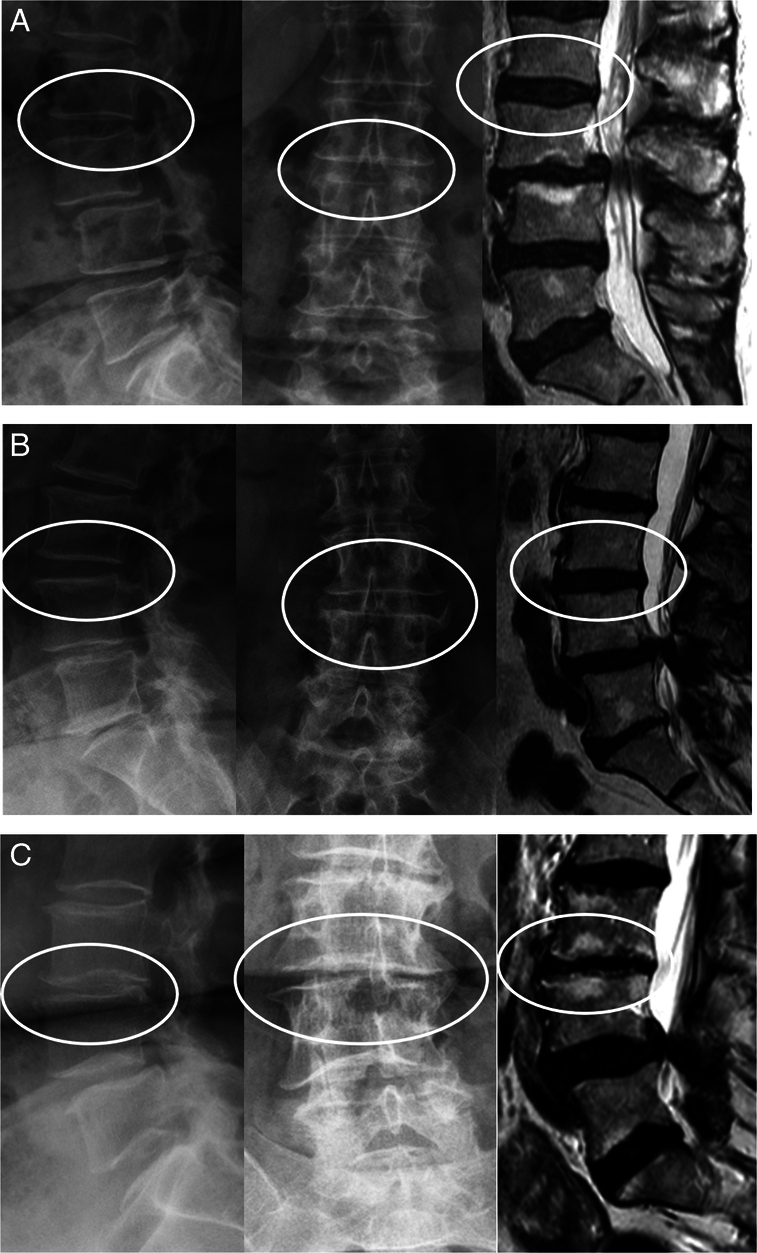
Summary of background data: ASD incurs late reoperations after lumbar fusion surgeries. ASD pathogenesis is multifactorial. Preexisting adjacent segment degeneration, measured by Pfirrmann, is suggested as one of the predisposing factors. We sought to find deeper insights into this association by using a more granular degeneration measure, the combined imaging score (CIS).
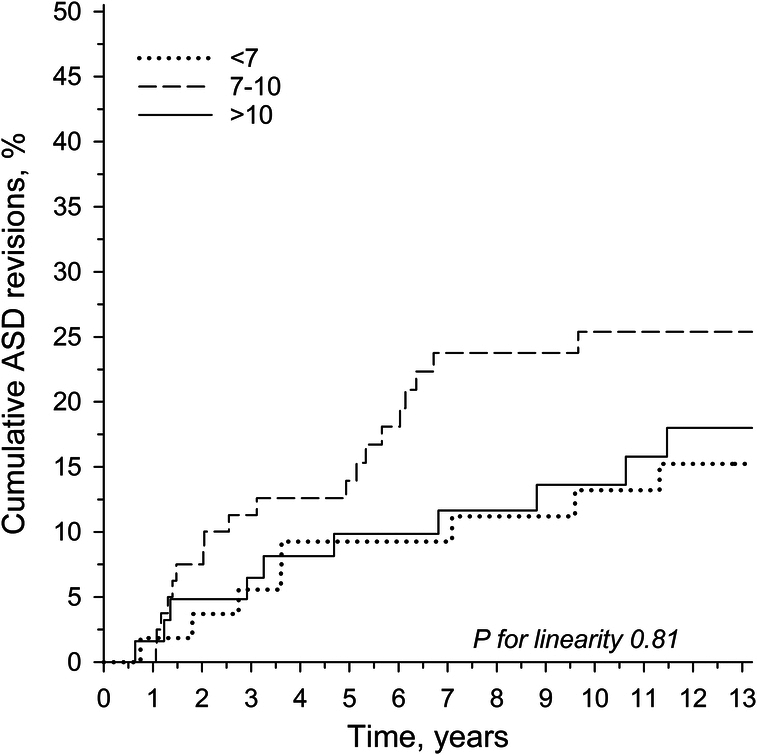
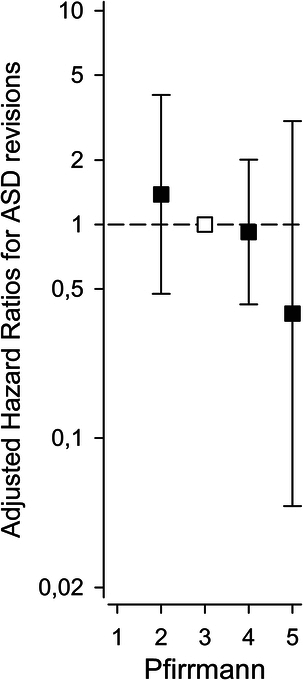
Patients and methods: A total of 197 consecutive lumbar fusions for degenerative pathologies were enrolled in a prospective follow-up (median: 12 yr). Preoperative cranial adjacent segment degeneration status was determined using Pfirrmann and CIS, which utilize both radiographs and magnetic resonance imaging. On the basis of CIS, patients were trichotomized into tertiles (CIS <7, CIS 7-10, and CIS >10). The cumulative ASD revision risk was determined for each tertile. After adjusting for age, sex, body mass index, sacral fixation, and fusion length, hazard ratios (95% CI) for ASD revisions were determined for each Pfirrmann and CIS score.
Results: Patients in the intermediate CIS tertile had a cumulative ASD revision risk of 25.4% (17.0%-37.0%), while both milder degeneration (CIS <7) [13.2% (6.5%-25.8%)] and end-stage degeneration (CIS >10) [13.6% (7.0%-25.5%)] appeared to be protective against surgical ASD. Pfirrmann failed to show a significant association with ASD revision risk. Adjusted analysis of CIS suggested increased ASD revisions after CIS 7, which turned contrariwise after CIS 10.
Conclusions: The effect of preexisting adjacent segment degeneration on ASD reoperation risk is not linear. The risk appears to increase with advancing degeneration but diminishes with end-stage degeneration. Therefore, end-stage degenerative segments may be considered to be excluded from fusion constructs.
期刊介绍:
Lippincott Williams & Wilkins is a leading international publisher of professional health information for physicians, nurses, specialized clinicians and students. For a complete listing of titles currently published by Lippincott Williams & Wilkins and detailed information about print, online, and other offerings, please visit the LWW Online Store.
Recognized internationally as the leading journal in its field, Spine is an international, peer-reviewed, bi-weekly periodical that considers for publication original articles in the field of Spine. It is the leading subspecialty journal for the treatment of spinal disorders. Only original papers are considered for publication with the understanding that they are contributed solely to Spine. The Journal does not publish articles reporting material that has been reported at length elsewhere.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
