John M Flack, Michael G Buhnerkempe, Kenneth Todd Moore
{"title":"耐药性高血压:疾病负担与新兴治疗方案。","authors":"John M Flack, Michael G Buhnerkempe, Kenneth Todd Moore","doi":"10.1007/s11906-023-01282-0","DOIUrl":null,"url":null,"abstract":"<p><strong>Purpose of review: </strong>To define resistant hypertension (RHT), review its pathophysiology and disease burden, identify barriers to effective hypertension management, and to highlight emerging treatment options.</p><p><strong>Recent findings: </strong>RHT is defined as uncontrolled blood pressure (BP) ≥ 130/80 mm Hg despite concurrent prescription of ≥ 3 or ≥ 4 antihypertensive drugs in different classes or controlled BP despite prescription of ≥ to 4 drugs, at maximally tolerated doses, including a diuretic. BP is regulated by a complex interplay between the renin-angiotensin-aldosterone system, the sympathetic nervous system, the endothelin system, natriuretic peptides, the arterial vasculature, and the immune system; disruption of any of these can increase BP. RHT is disproportionately manifest in African Americans, older patients, and those with diabetes and/or chronic kidney disease (CKD). Amongst drug-treated hypertensives, only one-quarter have been treated intensively enough (prescribed > 2 drugs) to be considered for this diagnosis. New treatment strategies aimed at novel therapeutic targets include inhibition of sodium-glucose cotransporter 2, aminopeptidase A, aldosterone synthesis, phosphodiesterase 5, xanthine oxidase, and dopamine beta-hydroxylase, as well as soluble guanylate cyclase stimulation, nonsteroidal mineralocorticoid receptor antagonism, and dual endothelin receptor antagonism. The burden of RHT remains high. Better use of currently approved therapies and integrating emerging therapies are welcome additions to the therapeutic armamentarium for addressing needs in high-risk aTRH patients.</p>","PeriodicalId":10963,"journal":{"name":"Current Hypertension Reports","volume":" ","pages":"183-199"},"PeriodicalIF":5.1000,"publicationDate":"2024-05-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11533979/pdf/","citationCount":"0","resultStr":"{\"title\":\"Resistant Hypertension: Disease Burden and Emerging Treatment Options.\",\"authors\":\"John M Flack, Michael G Buhnerkempe, Kenneth Todd Moore\",\"doi\":\"10.1007/s11906-023-01282-0\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Purpose of review: </strong>To define resistant hypertension (RHT), review its pathophysiology and disease burden, identify barriers to effective hypertension management, and to highlight emerging treatment options.</p><p><strong>Recent findings: </strong>RHT is defined as uncontrolled blood pressure (BP) ≥ 130/80 mm Hg despite concurrent prescription of ≥ 3 or ≥ 4 antihypertensive drugs in different classes or controlled BP despite prescription of ≥ to 4 drugs, at maximally tolerated doses, including a diuretic. BP is regulated by a complex interplay between the renin-angiotensin-aldosterone system, the sympathetic nervous system, the endothelin system, natriuretic peptides, the arterial vasculature, and the immune system; disruption of any of these can increase BP. RHT is disproportionately manifest in African Americans, older patients, and those with diabetes and/or chronic kidney disease (CKD). Amongst drug-treated hypertensives, only one-quarter have been treated intensively enough (prescribed > 2 drugs) to be considered for this diagnosis. New treatment strategies aimed at novel therapeutic targets include inhibition of sodium-glucose cotransporter 2, aminopeptidase A, aldosterone synthesis, phosphodiesterase 5, xanthine oxidase, and dopamine beta-hydroxylase, as well as soluble guanylate cyclase stimulation, nonsteroidal mineralocorticoid receptor antagonism, and dual endothelin receptor antagonism. The burden of RHT remains high. Better use of currently approved therapies and integrating emerging therapies are welcome additions to the therapeutic armamentarium for addressing needs in high-risk aTRH patients.</p>\",\"PeriodicalId\":10963,\"journal\":{\"name\":\"Current Hypertension Reports\",\"volume\":\" \",\"pages\":\"183-199\"},\"PeriodicalIF\":5.1000,\"publicationDate\":\"2024-05-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11533979/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Current Hypertension Reports\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1007/s11906-023-01282-0\",\"RegionNum\":2,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2024/2/16 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q1\",\"JCRName\":\"PERIPHERAL VASCULAR DISEASE\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Current Hypertension Reports","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1007/s11906-023-01282-0","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/2/16 0:00:00","PubModel":"Epub","JCR":"Q1","JCRName":"PERIPHERAL VASCULAR DISEASE","Score":null,"Total":0}
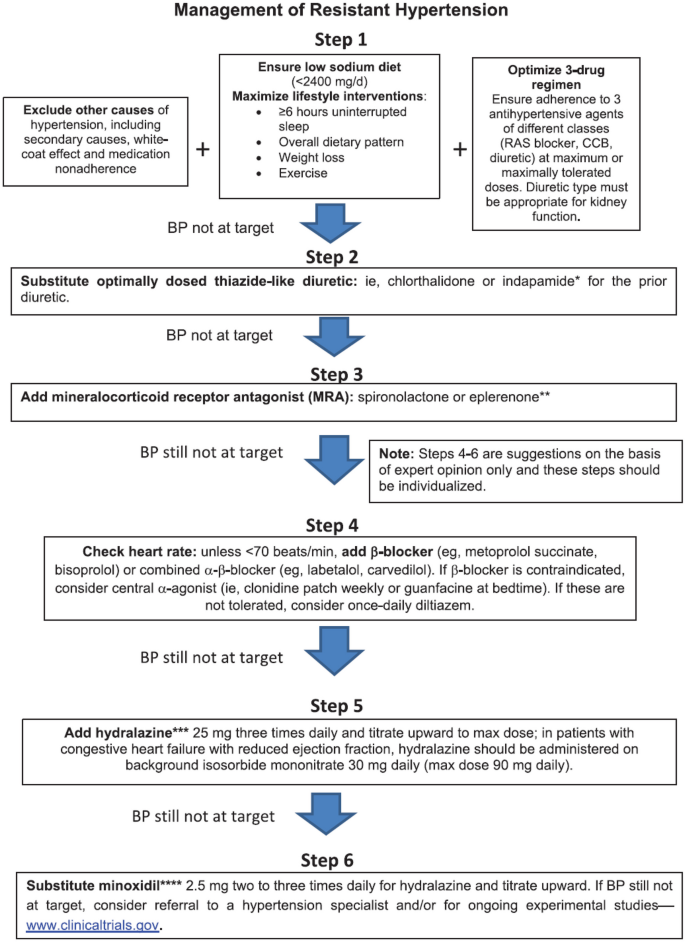
Resistant Hypertension: Disease Burden and Emerging Treatment Options.
Purpose of review: To define resistant hypertension (RHT), review its pathophysiology and disease burden, identify barriers to effective hypertension management, and to highlight emerging treatment options.
Recent findings: RHT is defined as uncontrolled blood pressure (BP) ≥ 130/80 mm Hg despite concurrent prescription of ≥ 3 or ≥ 4 antihypertensive drugs in different classes or controlled BP despite prescription of ≥ to 4 drugs, at maximally tolerated doses, including a diuretic. BP is regulated by a complex interplay between the renin-angiotensin-aldosterone system, the sympathetic nervous system, the endothelin system, natriuretic peptides, the arterial vasculature, and the immune system; disruption of any of these can increase BP. RHT is disproportionately manifest in African Americans, older patients, and those with diabetes and/or chronic kidney disease (CKD). Amongst drug-treated hypertensives, only one-quarter have been treated intensively enough (prescribed > 2 drugs) to be considered for this diagnosis. New treatment strategies aimed at novel therapeutic targets include inhibition of sodium-glucose cotransporter 2, aminopeptidase A, aldosterone synthesis, phosphodiesterase 5, xanthine oxidase, and dopamine beta-hydroxylase, as well as soluble guanylate cyclase stimulation, nonsteroidal mineralocorticoid receptor antagonism, and dual endothelin receptor antagonism. The burden of RHT remains high. Better use of currently approved therapies and integrating emerging therapies are welcome additions to the therapeutic armamentarium for addressing needs in high-risk aTRH patients.
期刊介绍:
This journal intends to provide clear, insightful, balanced contributions by international experts that review the most important, recently published clinical findings related to the diagnosis, treatment, management, and prevention of hypertension.
We accomplish this aim by appointing international authorities to serve as Section Editors in key subject areas, such as antihypertensive therapies, associated metabolic disorders, and therapeutic trials. Section Editors, in turn, select topics for which leading experts contribute comprehensive review articles that emphasize new developments and recently published papers of major importance, highlighted by annotated reference lists. An international Editorial Board reviews the annual table of contents, suggests articles of special interest to their country/region, and ensures that topics are current and include emerging research. Commentaries from well-known figures in the field are also provided.


 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
