Go Hashimoto MD , Santiago Garcia MD , Hirotomo Sato MD, PhD , Miho Fukui MD, PhD , Muhammad Hammadah MD , Robert Steffen MD , Joao L. Cavalcante MD , Vinayak N. Bapat MD
{"title":"从台架测试和计算机断层扫描分析中获得生物人工瓣膜断裂的新见解和新视角","authors":"Go Hashimoto MD , Santiago Garcia MD , Hirotomo Sato MD, PhD , Miho Fukui MD, PhD , Muhammad Hammadah MD , Robert Steffen MD , Joao L. Cavalcante MD , Vinayak N. Bapat MD","doi":"10.1016/j.shj.2023.100276","DOIUrl":null,"url":null,"abstract":"<div><h3>Background</h3><p>Bioprosthetic valve fracture (BVF) during valve-in-valve TAVR (transcatheter aortic valve replacement) is a procedural adjunct designed to optimize the expansion of the transcatheter heart valve and reduce patient-prosthesis mismatch by using a high-pressure balloon to intentionally fracture the surgical heart valve (SHV).</p></div><div><h3>Methods</h3><p>We performed bench testing on 15 bioprosthetic SHV to examine the optimal balloon size and pressure for BVF. We assessed morphological changes and expansion of SHV by computed tomography angiography. Successful BVF was defined as balloon waist disappearance on fluoroscopy and/or sudden pressure drop during balloon inflation.</p></div><div><h3>Results</h3><p>Nine valves met the definition of BVF, 3 of which were confirmed by disruption of the stent frame. We classified surgical valves into 3 subsets: 1) fracturable with metal stent frame (MSF), 2) fracturable with polymer stent frame (PSF) and 3) nonfracturable. In general, valves with MSF were fractured using a balloon size = true internal diameter plus 3-5 mm inflated at high pressure (16-20 ATM) whereas valves with PSF could be fractured with a balloon size = true internal diameter plus 3-5 mm and lower balloon pressure (6-14 ATM). Gains in computed tomography angiography derived inflow area after BVF were 12.3% for MSF and 3.6% for PSF SHV.</p></div><div><h3>Conclusions</h3><p>Gains in CT-determined valve area after BVF depend on the physical properties of the SHV, which in turn influences pressure thresholds and balloon sizing strategy for optimal BVF. Elastic recoil of PSF valves limits the gains in inflow area after BVF.</p></div>","PeriodicalId":36053,"journal":{"name":"Structural Heart","volume":"8 3","pages":"Article 100276"},"PeriodicalIF":2.8000,"publicationDate":"2024-05-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.sciencedirect.com/science/article/pii/S2474870623002270/pdfft?md5=dc4b4504d617eb1cce9871314a0e5ed4&pid=1-s2.0-S2474870623002270-main.pdf","citationCount":"0","resultStr":"{\"title\":\"New Insights and Perspective on Bioprosthetic Valve Fracture From Bench Testing and Computed Tomography Analysis\",\"authors\":\"Go Hashimoto MD , Santiago Garcia MD , Hirotomo Sato MD, PhD , Miho Fukui MD, PhD , Muhammad Hammadah MD , Robert Steffen MD , Joao L. Cavalcante MD , Vinayak N. Bapat MD\",\"doi\":\"10.1016/j.shj.2023.100276\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<div><h3>Background</h3><p>Bioprosthetic valve fracture (BVF) during valve-in-valve TAVR (transcatheter aortic valve replacement) is a procedural adjunct designed to optimize the expansion of the transcatheter heart valve and reduce patient-prosthesis mismatch by using a high-pressure balloon to intentionally fracture the surgical heart valve (SHV).</p></div><div><h3>Methods</h3><p>We performed bench testing on 15 bioprosthetic SHV to examine the optimal balloon size and pressure for BVF. We assessed morphological changes and expansion of SHV by computed tomography angiography. Successful BVF was defined as balloon waist disappearance on fluoroscopy and/or sudden pressure drop during balloon inflation.</p></div><div><h3>Results</h3><p>Nine valves met the definition of BVF, 3 of which were confirmed by disruption of the stent frame. We classified surgical valves into 3 subsets: 1) fracturable with metal stent frame (MSF), 2) fracturable with polymer stent frame (PSF) and 3) nonfracturable. In general, valves with MSF were fractured using a balloon size = true internal diameter plus 3-5 mm inflated at high pressure (16-20 ATM) whereas valves with PSF could be fractured with a balloon size = true internal diameter plus 3-5 mm and lower balloon pressure (6-14 ATM). Gains in computed tomography angiography derived inflow area after BVF were 12.3% for MSF and 3.6% for PSF SHV.</p></div><div><h3>Conclusions</h3><p>Gains in CT-determined valve area after BVF depend on the physical properties of the SHV, which in turn influences pressure thresholds and balloon sizing strategy for optimal BVF. Elastic recoil of PSF valves limits the gains in inflow area after BVF.</p></div>\",\"PeriodicalId\":36053,\"journal\":{\"name\":\"Structural Heart\",\"volume\":\"8 3\",\"pages\":\"Article 100276\"},\"PeriodicalIF\":2.8000,\"publicationDate\":\"2024-05-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.sciencedirect.com/science/article/pii/S2474870623002270/pdfft?md5=dc4b4504d617eb1cce9871314a0e5ed4&pid=1-s2.0-S2474870623002270-main.pdf\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Structural Heart\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://www.sciencedirect.com/science/article/pii/S2474870623002270\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2024/2/5 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q3\",\"JCRName\":\"CARDIAC & CARDIOVASCULAR SYSTEMS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Structural Heart","FirstCategoryId":"1085","ListUrlMain":"https://www.sciencedirect.com/science/article/pii/S2474870623002270","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/2/5 0:00:00","PubModel":"Epub","JCR":"Q3","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
New Insights and Perspective on Bioprosthetic Valve Fracture From Bench Testing and Computed Tomography Analysis
Background
Bioprosthetic valve fracture (BVF) during valve-in-valve TAVR (transcatheter aortic valve replacement) is a procedural adjunct designed to optimize the expansion of the transcatheter heart valve and reduce patient-prosthesis mismatch by using a high-pressure balloon to intentionally fracture the surgical heart valve (SHV).
Methods
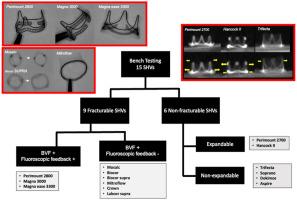
We performed bench testing on 15 bioprosthetic SHV to examine the optimal balloon size and pressure for BVF. We assessed morphological changes and expansion of SHV by computed tomography angiography. Successful BVF was defined as balloon waist disappearance on fluoroscopy and/or sudden pressure drop during balloon inflation.
Results
Nine valves met the definition of BVF, 3 of which were confirmed by disruption of the stent frame. We classified surgical valves into 3 subsets: 1) fracturable with metal stent frame (MSF), 2) fracturable with polymer stent frame (PSF) and 3) nonfracturable. In general, valves with MSF were fractured using a balloon size = true internal diameter plus 3-5 mm inflated at high pressure (16-20 ATM) whereas valves with PSF could be fractured with a balloon size = true internal diameter plus 3-5 mm and lower balloon pressure (6-14 ATM). Gains in computed tomography angiography derived inflow area after BVF were 12.3% for MSF and 3.6% for PSF SHV.
Conclusions
Gains in CT-determined valve area after BVF depend on the physical properties of the SHV, which in turn influences pressure thresholds and balloon sizing strategy for optimal BVF. Elastic recoil of PSF valves limits the gains in inflow area after BVF.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
