Jiaqi Cai, Ming Yang, Han Deng, Hao Bai, Guanhao Zheng, Juan He
{"title":"急性肾损伤不容忽视--预测血流感染重症患者死亡率的快速皮特菌血症评分的优化:一项回顾性队列研究。","authors":"Jiaqi Cai, Ming Yang, Han Deng, Hao Bai, Guanhao Zheng, Juan He","doi":"10.1177/20499361241231147","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Considering the therapeutic difficulties and mortality associated with bloodstream infection (BSI), it is essential to investigate other potential factors affecting mortality in critically ill patients with BSI and examine the utility of the quick Pitt bacteremia (qPitt) score to improve the survival rate.</p><p><strong>Objectives: </strong>To improve the predictive accuracy of the qPitt scoring system by evaluating the five current components of qPitt and including other potential factors influencing mortality in critically ill patients with BSI.</p><p><strong>Design: </strong>This was a retrospective cohort study.</p><p><strong>Methods: </strong>Medical information from the Medical Information Mart for Intensive Care IV database was used in this retrospective cohort study. The risk factors associated with mortality were examined using a multivariate logistic regression model. The area under the receiver operating characteristic curve (AUC) was used to assess the discriminatory capability of the prediction models.</p><p><strong>Results: </strong>In total, 1240 eligible critically ill patients with BSI were included. After adjustment for age, community-onset BSI, indwelling invasive lines, and Glasgow Coma Scale (GCS) ⩽ 8, acute kidney injury (AKI) was identified as a notable risk factor for 14-day mortality. Except for altered mental status, the four other main components of the original qPitt were significantly associated with 14-day mortality. Hence, we established a modified qPitt (m-qPitt) by adding AKI and replacing altered mental status with GCS ⩽ 8. The AUCs for m-qPitt and qPitt were 0.723 [95% confidence interval (CI): 0.683-0.759] and 0.708 (95% CI: 0.669-0.745) in predicting 14-day mortality, respectively. Moreover, m-qPitt also had acceptable performance and discrimination power [0.700 (95% CI: 0.666-0.732)] in predicting 28-day mortality.</p><p><strong>Conclusion: </strong>AKI significantly influenced the survival of critically ill patients with BSIs. Compared with the original qPitt, our new m-qPitt was proven to have a better predictive performance for mortality in critically ill patients with BSI. Further studies should be conducted to validate the practicality of m-qPitt.</p>","PeriodicalId":46154,"journal":{"name":"Therapeutic Advances in Infectious Disease","volume":"11 ","pages":"20499361241231147"},"PeriodicalIF":3.4000,"publicationDate":"2024-02-23","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10896049/pdf/","citationCount":"0","resultStr":"{\"title\":\"Acute kidney injury should not be neglected - optimization of quick Pitt bacteremia score for predicting mortality in critically ill patients with bloodstream infection: a retrospective cohort study.\",\"authors\":\"Jiaqi Cai, Ming Yang, Han Deng, Hao Bai, Guanhao Zheng, Juan He\",\"doi\":\"10.1177/20499361241231147\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Considering the therapeutic difficulties and mortality associated with bloodstream infection (BSI), it is essential to investigate other potential factors affecting mortality in critically ill patients with BSI and examine the utility of the quick Pitt bacteremia (qPitt) score to improve the survival rate.</p><p><strong>Objectives: </strong>To improve the predictive accuracy of the qPitt scoring system by evaluating the five current components of qPitt and including other potential factors influencing mortality in critically ill patients with BSI.</p><p><strong>Design: </strong>This was a retrospective cohort study.</p><p><strong>Methods: </strong>Medical information from the Medical Information Mart for Intensive Care IV database was used in this retrospective cohort study. The risk factors associated with mortality were examined using a multivariate logistic regression model. The area under the receiver operating characteristic curve (AUC) was used to assess the discriminatory capability of the prediction models.</p><p><strong>Results: </strong>In total, 1240 eligible critically ill patients with BSI were included. After adjustment for age, community-onset BSI, indwelling invasive lines, and Glasgow Coma Scale (GCS) ⩽ 8, acute kidney injury (AKI) was identified as a notable risk factor for 14-day mortality. Except for altered mental status, the four other main components of the original qPitt were significantly associated with 14-day mortality. Hence, we established a modified qPitt (m-qPitt) by adding AKI and replacing altered mental status with GCS ⩽ 8. The AUCs for m-qPitt and qPitt were 0.723 [95% confidence interval (CI): 0.683-0.759] and 0.708 (95% CI: 0.669-0.745) in predicting 14-day mortality, respectively. Moreover, m-qPitt also had acceptable performance and discrimination power [0.700 (95% CI: 0.666-0.732)] in predicting 28-day mortality.</p><p><strong>Conclusion: </strong>AKI significantly influenced the survival of critically ill patients with BSIs. Compared with the original qPitt, our new m-qPitt was proven to have a better predictive performance for mortality in critically ill patients with BSI. Further studies should be conducted to validate the practicality of m-qPitt.</p>\",\"PeriodicalId\":46154,\"journal\":{\"name\":\"Therapeutic Advances in Infectious Disease\",\"volume\":\"11 \",\"pages\":\"20499361241231147\"},\"PeriodicalIF\":3.4000,\"publicationDate\":\"2024-02-23\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10896049/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Therapeutic Advances in Infectious Disease\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1177/20499361241231147\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2024/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q2\",\"JCRName\":\"INFECTIOUS DISEASES\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Therapeutic Advances in Infectious Disease","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1177/20499361241231147","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/1/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"INFECTIOUS DISEASES","Score":null,"Total":0}
Acute kidney injury should not be neglected - optimization of quick Pitt bacteremia score for predicting mortality in critically ill patients with bloodstream infection: a retrospective cohort study.
Background: Considering the therapeutic difficulties and mortality associated with bloodstream infection (BSI), it is essential to investigate other potential factors affecting mortality in critically ill patients with BSI and examine the utility of the quick Pitt bacteremia (qPitt) score to improve the survival rate.
Objectives: To improve the predictive accuracy of the qPitt scoring system by evaluating the five current components of qPitt and including other potential factors influencing mortality in critically ill patients with BSI.
Design: This was a retrospective cohort study.
Methods: Medical information from the Medical Information Mart for Intensive Care IV database was used in this retrospective cohort study. The risk factors associated with mortality were examined using a multivariate logistic regression model. The area under the receiver operating characteristic curve (AUC) was used to assess the discriminatory capability of the prediction models.
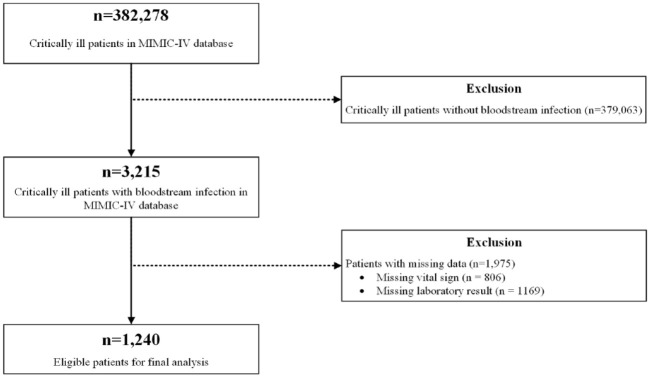
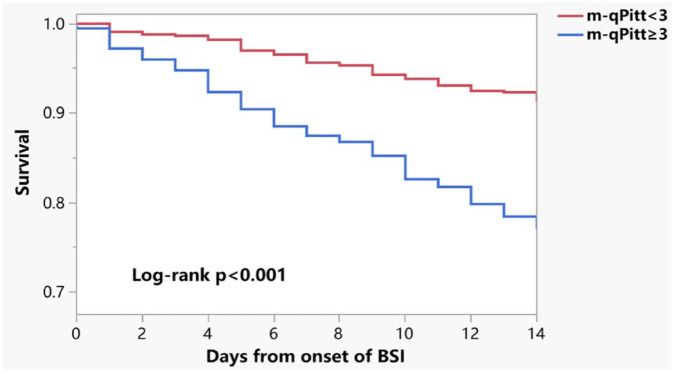
Results: In total, 1240 eligible critically ill patients with BSI were included. After adjustment for age, community-onset BSI, indwelling invasive lines, and Glasgow Coma Scale (GCS) ⩽ 8, acute kidney injury (AKI) was identified as a notable risk factor for 14-day mortality. Except for altered mental status, the four other main components of the original qPitt were significantly associated with 14-day mortality. Hence, we established a modified qPitt (m-qPitt) by adding AKI and replacing altered mental status with GCS ⩽ 8. The AUCs for m-qPitt and qPitt were 0.723 [95% confidence interval (CI): 0.683-0.759] and 0.708 (95% CI: 0.669-0.745) in predicting 14-day mortality, respectively. Moreover, m-qPitt also had acceptable performance and discrimination power [0.700 (95% CI: 0.666-0.732)] in predicting 28-day mortality.
Conclusion: AKI significantly influenced the survival of critically ill patients with BSIs. Compared with the original qPitt, our new m-qPitt was proven to have a better predictive performance for mortality in critically ill patients with BSI. Further studies should be conducted to validate the practicality of m-qPitt.





 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
