Sanjaya Gupta, Raghu Kolluri, Tiessa Simoes, Sandeep C Pingle, Hong Nie, Michael S Lloyd, Daniel Steinhaus, Stacy B Westerman, Anand Shah, Jessica Kline, Soroosh Kiani
{"title":"心房颤动和扑动导管消融术后多入口静脉闭合的安全性。","authors":"Sanjaya Gupta, Raghu Kolluri, Tiessa Simoes, Sandeep C Pingle, Hong Nie, Michael S Lloyd, Daniel Steinhaus, Stacy B Westerman, Anand Shah, Jessica Kline, Soroosh Kiani","doi":"10.1007/s10840-024-01773-3","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Following catheter ablation, vascular access management involves potential complications and prolonged recovery. Recently, suture-mediated closure (SMC) devices were approved for venous access procedures. The objective of this study is to evaluate the safety of a commercially available SMC for multiple access site venous closure by duplex ultrasound (DUS) in asymptomatic subjects with non-visible complications.</p><p><strong>Methods: </strong>Thirty-six subjects (63 ± 10.7 years old, 12 female) were enrolled. Following catheter ablation for atrial fibrillation, all subjects had SMC of every venous access site. Subjects underwent DUS of femoral veins and arteries. DUS was performed at discharge, and again at 30 days. Subjects were evaluated for clinically apparent vascular complications.</p><p><strong>Results: </strong>Mean procedure duration was 138.6 min, and the time to hemostasis was 3.1 min/access site and 9.5 min/subject. Median time to ambulation was 193.5 min, and median time to discharge was 5.95 h, with discharge as early as 2.4 h. A median of 2 sheaths/vein and a median of 2 SMC devices/vein were used. There were no major complications and a 16.7% (6/36) minor complication rate at discharge. All complications resolved at 30 days. The complication rate was not higher in patients with 2 SMC per access site as compared to the patients who just received 1 SMC per access site.</p><p><strong>Conclusions: </strong>This study demonstrates the safety of multi-access closure using SMC, following catheter ablation procedures, for closure of sites that use sheath sizes from ≤ 8F to ≥ 15F and for those that use 2 or more SMCs per access site.</p>","PeriodicalId":16202,"journal":{"name":"Journal of Interventional Cardiac Electrophysiology","volume":" ","pages":"1437-1443"},"PeriodicalIF":2.6000,"publicationDate":"2024-09-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11379729/pdf/","citationCount":"0","resultStr":"{\"title\":\"Safety of multi-access site venous closure following catheter ablation of atrial fibrillation and flutter.\",\"authors\":\"Sanjaya Gupta, Raghu Kolluri, Tiessa Simoes, Sandeep C Pingle, Hong Nie, Michael S Lloyd, Daniel Steinhaus, Stacy B Westerman, Anand Shah, Jessica Kline, Soroosh Kiani\",\"doi\":\"10.1007/s10840-024-01773-3\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Following catheter ablation, vascular access management involves potential complications and prolonged recovery. Recently, suture-mediated closure (SMC) devices were approved for venous access procedures. The objective of this study is to evaluate the safety of a commercially available SMC for multiple access site venous closure by duplex ultrasound (DUS) in asymptomatic subjects with non-visible complications.</p><p><strong>Methods: </strong>Thirty-six subjects (63 ± 10.7 years old, 12 female) were enrolled. Following catheter ablation for atrial fibrillation, all subjects had SMC of every venous access site. Subjects underwent DUS of femoral veins and arteries. DUS was performed at discharge, and again at 30 days. Subjects were evaluated for clinically apparent vascular complications.</p><p><strong>Results: </strong>Mean procedure duration was 138.6 min, and the time to hemostasis was 3.1 min/access site and 9.5 min/subject. Median time to ambulation was 193.5 min, and median time to discharge was 5.95 h, with discharge as early as 2.4 h. A median of 2 sheaths/vein and a median of 2 SMC devices/vein were used. There were no major complications and a 16.7% (6/36) minor complication rate at discharge. All complications resolved at 30 days. The complication rate was not higher in patients with 2 SMC per access site as compared to the patients who just received 1 SMC per access site.</p><p><strong>Conclusions: </strong>This study demonstrates the safety of multi-access closure using SMC, following catheter ablation procedures, for closure of sites that use sheath sizes from ≤ 8F to ≥ 15F and for those that use 2 or more SMCs per access site.</p>\",\"PeriodicalId\":16202,\"journal\":{\"name\":\"Journal of Interventional Cardiac Electrophysiology\",\"volume\":\" \",\"pages\":\"1437-1443\"},\"PeriodicalIF\":2.6000,\"publicationDate\":\"2024-09-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11379729/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of Interventional Cardiac Electrophysiology\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1007/s10840-024-01773-3\",\"RegionNum\":4,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2024/2/27 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q3\",\"JCRName\":\"CARDIAC & CARDIOVASCULAR SYSTEMS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Interventional Cardiac Electrophysiology","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1007/s10840-024-01773-3","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/2/27 0:00:00","PubModel":"Epub","JCR":"Q3","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
Safety of multi-access site venous closure following catheter ablation of atrial fibrillation and flutter.
Background: Following catheter ablation, vascular access management involves potential complications and prolonged recovery. Recently, suture-mediated closure (SMC) devices were approved for venous access procedures. The objective of this study is to evaluate the safety of a commercially available SMC for multiple access site venous closure by duplex ultrasound (DUS) in asymptomatic subjects with non-visible complications.
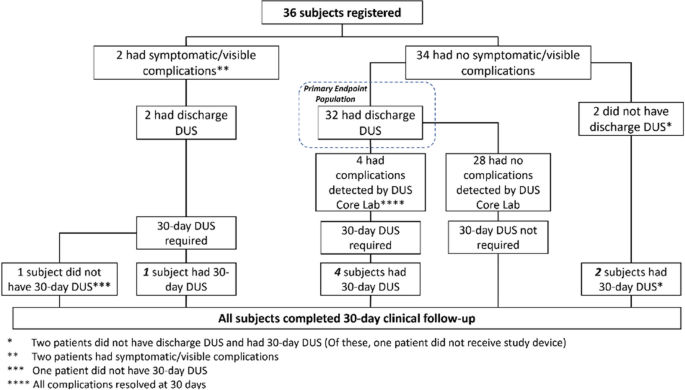
Methods: Thirty-six subjects (63 ± 10.7 years old, 12 female) were enrolled. Following catheter ablation for atrial fibrillation, all subjects had SMC of every venous access site. Subjects underwent DUS of femoral veins and arteries. DUS was performed at discharge, and again at 30 days. Subjects were evaluated for clinically apparent vascular complications.
Results: Mean procedure duration was 138.6 min, and the time to hemostasis was 3.1 min/access site and 9.5 min/subject. Median time to ambulation was 193.5 min, and median time to discharge was 5.95 h, with discharge as early as 2.4 h. A median of 2 sheaths/vein and a median of 2 SMC devices/vein were used. There were no major complications and a 16.7% (6/36) minor complication rate at discharge. All complications resolved at 30 days. The complication rate was not higher in patients with 2 SMC per access site as compared to the patients who just received 1 SMC per access site.
Conclusions: This study demonstrates the safety of multi-access closure using SMC, following catheter ablation procedures, for closure of sites that use sheath sizes from ≤ 8F to ≥ 15F and for those that use 2 or more SMCs per access site.
期刊介绍:
The Journal of Interventional Cardiac Electrophysiology is an international publication devoted to fostering research in and development of interventional techniques and therapies for the management of cardiac arrhythmias. It is designed primarily to present original research studies and scholarly scientific reviews of basic and applied science and clinical research in this field. The Journal will adopt a multidisciplinary approach to link physical, experimental, and clinical sciences as applied to the development of and practice in interventional electrophysiology. The Journal will examine techniques ranging from molecular, chemical and pharmacologic therapies to device and ablation technology. Accordingly, original research in clinical, epidemiologic and basic science arenas will be considered for publication. Applied engineering or physical science studies pertaining to interventional electrophysiology will be encouraged. The Journal is committed to providing comprehensive and detailed treatment of major interventional therapies and innovative techniques in a structured and clinically relevant manner. It is directed at clinical practitioners and investigators in the rapidly growing field of interventional electrophysiology. The editorial staff and board reflect this bias and include noted international experts in this area with a wealth of expertise in basic and clinical investigation. Peer review of all submissions, conflict of interest guidelines and periodic editorial board review of all Journal policies have been established.



 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
