{"title":"股骨干病变的重复药物涂层球囊血管成形术:一项回顾性观察研究的 12 个月结果。","authors":"Takuya Haraguchi, Masanaga Tsujimoto, Yoshifumi Kashima, Katsuhiko Sato, Tsutomu Fujita","doi":"10.1186/s42155-024-00434-w","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>The clinical implications of restenosis after drug-coated balloon (DCB) treatment remain unclear. We compared the clinical outcomes between DCB angioplasty for restenosis and de novo femoropopliteal artery lesions. This single-center retrospective study included 571 patients (737 limbs) who underwent either repeat (54 patients, 64 limbs) or de novo DCB (517 patients, 673 limbs) without bailout stenting. After propensity score matching, 49 matched pairs were analyzed. The primary endpoint was the 1-year primary patency, with secondary endpoints including the freedom from target lesion revascularization (TLR), major adverse limb events (MALE), and early restenosis. Predictors of restenosis were identified using multivariable Cox regression analysis.</p><p><strong>Results: </strong>The repeat-DCB group displayed significantly lower rates of 1-year primary patency and freedom from TLR compared to those of the de novo-DCB group (50.1% vs. 77.4%, p = 0.029 and 54.9% vs. 83.6%, p = 0.0.44, respectively). No significant differences were observed in early restenosis or MALE (10.7% vs. 5.9%, p = 0.455 and 48.3% vs. 73.4%, p = 0.055, respectively). Restenosis after DCB angioplasty was associated with repeat DCB (hazard ratio [HR], 5.13; 95% confidence interval [CI], 1.43-18.4; p = 0.012) and small vessel size of < 4.5 mm (HR, 6.25; 95% CI, 1.17-33.4; p = 0.032). Furthermore, restenosis after repeat DCB angioplasty was associated with the Peripheral Artery Calcification Scoring System (PACSS) grade 4 (HR, 4.20; 95% CI, 1.08-16.3; p = 0.038), small vessel size of < 4.5 mm (HR, 9.44; 95% CI, 1.21-73.7; p = 0.032), and intravascular ultrasound (IVUS) use (HR, 0.05; 95% CI, 0.01-0.44; p = 0.007).</p><p><strong>Conclusions: </strong>The 1-year primary patency rate following repeat DCB angioplasty for femoropopliteal lesions was notably lower than that of DCB treatment for de novo lesions. Repeat DCB strategy was associated with an increased risk of patency loss. Regarding repeat restenosis after DCB treatments, PACSS grade 4 calcification and small vessel diameter of < 4.5 mm were associated with an increased risk of restenosis, whereas IVUS use correlated with a decreased risk of restenosis.</p>","PeriodicalId":52351,"journal":{"name":"CVIR Endovascular","volume":"7 1","pages":"24"},"PeriodicalIF":2.1000,"publicationDate":"2024-02-29","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10904691/pdf/","citationCount":"0","resultStr":"{\"title\":\"Repeat drug-coated balloon angioplasty for femoropopliteal lesions: 12-month results from a retrospective observational study.\",\"authors\":\"Takuya Haraguchi, Masanaga Tsujimoto, Yoshifumi Kashima, Katsuhiko Sato, Tsutomu Fujita\",\"doi\":\"10.1186/s42155-024-00434-w\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>The clinical implications of restenosis after drug-coated balloon (DCB) treatment remain unclear. We compared the clinical outcomes between DCB angioplasty for restenosis and de novo femoropopliteal artery lesions. This single-center retrospective study included 571 patients (737 limbs) who underwent either repeat (54 patients, 64 limbs) or de novo DCB (517 patients, 673 limbs) without bailout stenting. After propensity score matching, 49 matched pairs were analyzed. The primary endpoint was the 1-year primary patency, with secondary endpoints including the freedom from target lesion revascularization (TLR), major adverse limb events (MALE), and early restenosis. Predictors of restenosis were identified using multivariable Cox regression analysis.</p><p><strong>Results: </strong>The repeat-DCB group displayed significantly lower rates of 1-year primary patency and freedom from TLR compared to those of the de novo-DCB group (50.1% vs. 77.4%, p = 0.029 and 54.9% vs. 83.6%, p = 0.0.44, respectively). No significant differences were observed in early restenosis or MALE (10.7% vs. 5.9%, p = 0.455 and 48.3% vs. 73.4%, p = 0.055, respectively). Restenosis after DCB angioplasty was associated with repeat DCB (hazard ratio [HR], 5.13; 95% confidence interval [CI], 1.43-18.4; p = 0.012) and small vessel size of < 4.5 mm (HR, 6.25; 95% CI, 1.17-33.4; p = 0.032). Furthermore, restenosis after repeat DCB angioplasty was associated with the Peripheral Artery Calcification Scoring System (PACSS) grade 4 (HR, 4.20; 95% CI, 1.08-16.3; p = 0.038), small vessel size of < 4.5 mm (HR, 9.44; 95% CI, 1.21-73.7; p = 0.032), and intravascular ultrasound (IVUS) use (HR, 0.05; 95% CI, 0.01-0.44; p = 0.007).</p><p><strong>Conclusions: </strong>The 1-year primary patency rate following repeat DCB angioplasty for femoropopliteal lesions was notably lower than that of DCB treatment for de novo lesions. Repeat DCB strategy was associated with an increased risk of patency loss. Regarding repeat restenosis after DCB treatments, PACSS grade 4 calcification and small vessel diameter of < 4.5 mm were associated with an increased risk of restenosis, whereas IVUS use correlated with a decreased risk of restenosis.</p>\",\"PeriodicalId\":52351,\"journal\":{\"name\":\"CVIR Endovascular\",\"volume\":\"7 1\",\"pages\":\"24\"},\"PeriodicalIF\":2.1000,\"publicationDate\":\"2024-02-29\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10904691/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"CVIR Endovascular\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1186/s42155-024-00434-w\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q3\",\"JCRName\":\"CARDIAC & CARDIOVASCULAR SYSTEMS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"CVIR Endovascular","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1186/s42155-024-00434-w","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
引用次数: 0
摘要
背景:药物涂层球囊(DCB)治疗后再狭窄的临床影响仍不明确。我们比较了DCB血管成形术治疗再狭窄和新生股腘动脉病变的临床效果。这项单中心回顾性研究纳入了 571 例患者(737 条肢体),他们接受了重复 DCB(54 例患者,64 条肢体)或从头 DCB(517 例患者,673 条肢体),均未接受保外支架治疗。经过倾向评分匹配后,对 49 对匹配患者进行了分析。主要终点是1年主要通畅率,次要终点包括靶病变血运重建(TLR)、肢体主要不良事件(MALE)和早期再狭窄。通过多变量考克斯回归分析确定了再狭窄的预测因素:结果:与新DCB组相比,重复DCB组的1年主要通畅率和无TLR率明显较低(分别为50.1% vs. 77.4%, p = 0.029和54.9% vs. 83.6%, p = 0.0.44)。在早期再狭窄或MALE方面未观察到明显差异(分别为10.7% vs. 5.9%,p = 0.455和48.3% vs. 73.4%,p = 0.055)。DCB血管成形术后的再狭窄与重复DCB(危险比[HR],5.13;95%置信区间[CI],1.43-18.4;P = 0.012)和结论的小血管尺寸有关:重复DCB血管成形术治疗股骨头病变后的1年初次通畅率明显低于DCB治疗新发病变。重复 DCB 策略与通畅损失风险增加有关。关于 DCB 治疗后的重复再狭窄,PACSS 4 级钙化和小血管直径为
Repeat drug-coated balloon angioplasty for femoropopliteal lesions: 12-month results from a retrospective observational study.
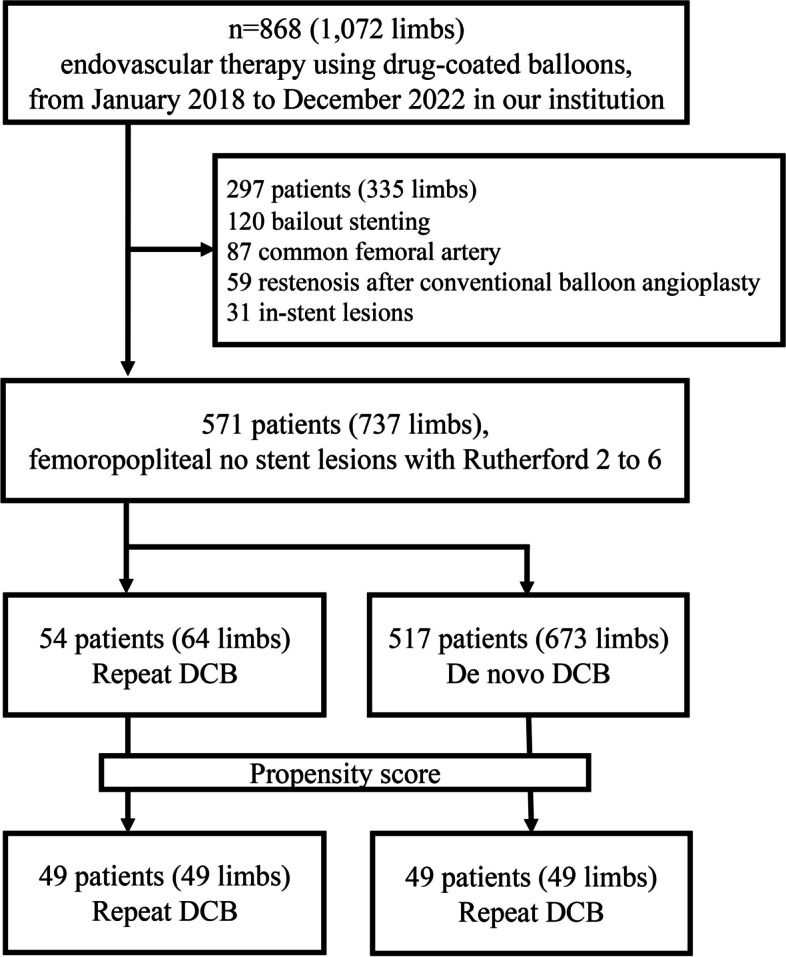
Background: The clinical implications of restenosis after drug-coated balloon (DCB) treatment remain unclear. We compared the clinical outcomes between DCB angioplasty for restenosis and de novo femoropopliteal artery lesions. This single-center retrospective study included 571 patients (737 limbs) who underwent either repeat (54 patients, 64 limbs) or de novo DCB (517 patients, 673 limbs) without bailout stenting. After propensity score matching, 49 matched pairs were analyzed. The primary endpoint was the 1-year primary patency, with secondary endpoints including the freedom from target lesion revascularization (TLR), major adverse limb events (MALE), and early restenosis. Predictors of restenosis were identified using multivariable Cox regression analysis.
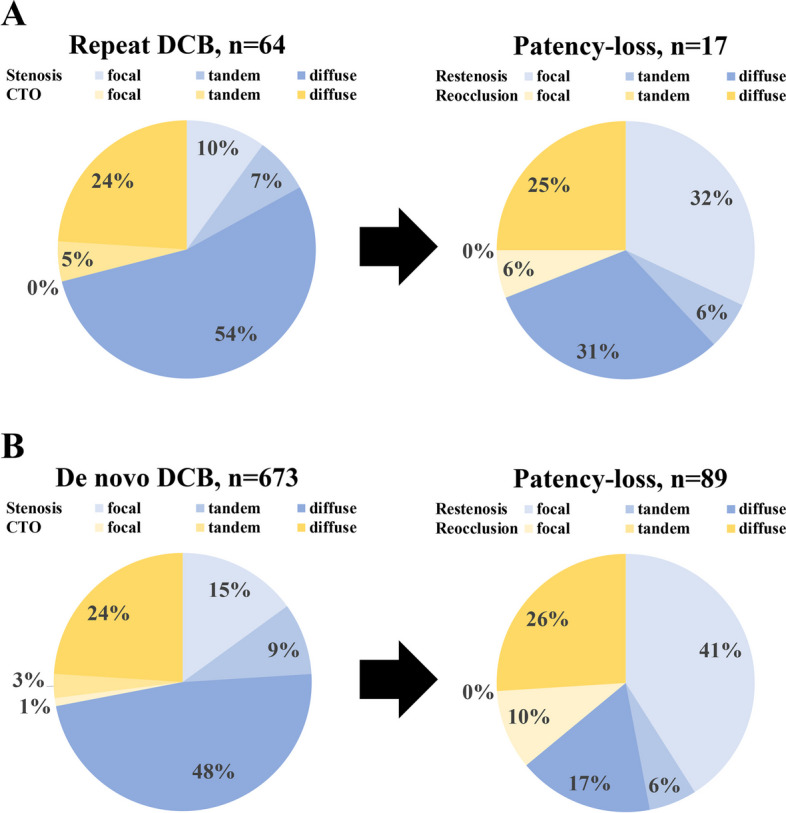
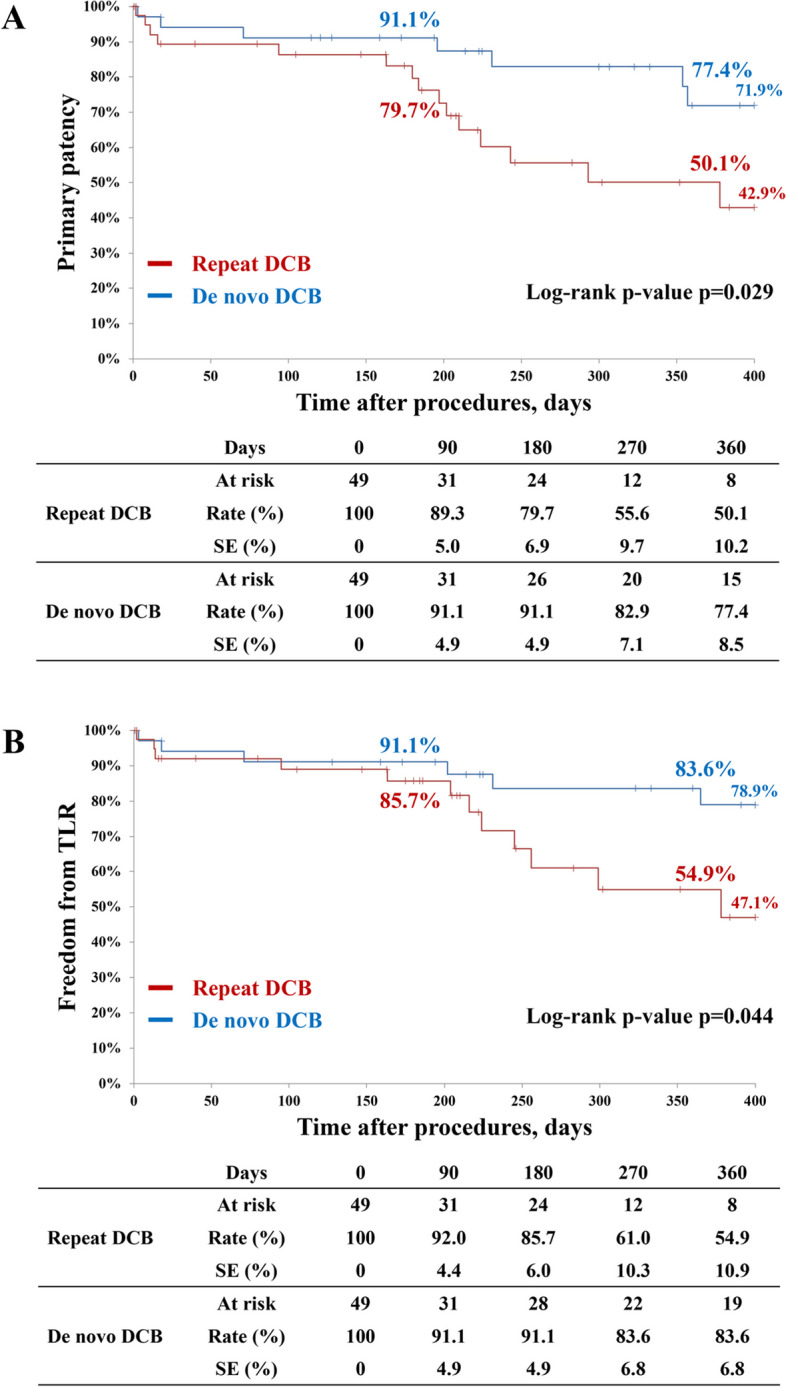
Results: The repeat-DCB group displayed significantly lower rates of 1-year primary patency and freedom from TLR compared to those of the de novo-DCB group (50.1% vs. 77.4%, p = 0.029 and 54.9% vs. 83.6%, p = 0.0.44, respectively). No significant differences were observed in early restenosis or MALE (10.7% vs. 5.9%, p = 0.455 and 48.3% vs. 73.4%, p = 0.055, respectively). Restenosis after DCB angioplasty was associated with repeat DCB (hazard ratio [HR], 5.13; 95% confidence interval [CI], 1.43-18.4; p = 0.012) and small vessel size of < 4.5 mm (HR, 6.25; 95% CI, 1.17-33.4; p = 0.032). Furthermore, restenosis after repeat DCB angioplasty was associated with the Peripheral Artery Calcification Scoring System (PACSS) grade 4 (HR, 4.20; 95% CI, 1.08-16.3; p = 0.038), small vessel size of < 4.5 mm (HR, 9.44; 95% CI, 1.21-73.7; p = 0.032), and intravascular ultrasound (IVUS) use (HR, 0.05; 95% CI, 0.01-0.44; p = 0.007).
Conclusions: The 1-year primary patency rate following repeat DCB angioplasty for femoropopliteal lesions was notably lower than that of DCB treatment for de novo lesions. Repeat DCB strategy was associated with an increased risk of patency loss. Regarding repeat restenosis after DCB treatments, PACSS grade 4 calcification and small vessel diameter of < 4.5 mm were associated with an increased risk of restenosis, whereas IVUS use correlated with a decreased risk of restenosis.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
