Meredith Hoog, Juan M Maldonado, Ruth Wangia-Dixon, Rachel Halpern, Erin Buysman, Garrett W Gremel, Ahong Huang, Manige Konig
{"title":"美国西班牙裔/拉美裔 2 型糖尿病患者使用度拉鲁肽与基础胰岛素的血糖和成本结果:一项真实世界研究。","authors":"Meredith Hoog, Juan M Maldonado, Ruth Wangia-Dixon, Rachel Halpern, Erin Buysman, Garrett W Gremel, Ahong Huang, Manige Konig","doi":"10.1007/s13300-024-01542-5","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>Optimal glycemic management after diabetes onset remains a challenge in Hispanic/Latino adults with type 2 diabetes (T2D), often resulting in poor health outcomes and higher rates of diabetes-related complications. The aim of this study was to examine and compare demographic and clinical characteristics, glycemic outcomes, health care resource utilization (HCRU), and costs among injection-naïve Hispanic/Latino adults with T2D initiating dulaglutide or basal insulin.</p><p><strong>Methods: </strong>This retrospective, observational study used administrative claims data from the Optum Research Database. Hispanic/Latino adults with T2D were assigned to dulaglutide or basal insulin cohorts on the basis of pharmacy claims and were propensity-score matched on demographic and baseline characteristics. Measures of glycemic management included 12 month follow-up glycated hemoglobin (HbA1c) and change in HbA1c from baseline. Follow-up all-cause and diabetes-related HCRU and costs, including costs per 1% change in HbA1c, were compared between cohorts.</p><p><strong>Results: </strong>The final propensity-score matched sample included 2872 patients: 1436 patients in each cohort. Mean (SD) reduction in HbA1c from baseline to 12 month follow-up was greater in the dulaglutide cohort compared with the basal insulin cohort [-1.40% (1.88) versus -0.92% (2.07); p < 0.001]. The dulaglutide cohort had significantly lower proportions of patients with ≥ 1 all-cause and diabetes-related outpatient visits, emergency room visits, and inpatient stays compared with the basal insulin cohort (p < 0.05). The dulaglutide cohort had significantly lower all-cause total costs per 1% HbA1c reduction than the basal insulin cohort ($13,768 versus $19,128; p < 0.001). Diabetes-related costs per 1% reduction were numerically lower for the dulaglutide cohort, but the difference was not statistically significant ($9737 versus $11,403; p = 0.081).</p><p><strong>Conclusions: </strong>Dulaglutide demonstrated better glycemic outcomes and lower all-cause costs per 1% HbA1c reduction among Hispanic/Latino adults compared with those initiating basal insulin. Our real-world findings in the Hispanic/Latino population were consistent with results obtained from the overall population and confirm the glycemic benefits of dulaglutide observed in clinical settings.</p>","PeriodicalId":11192,"journal":{"name":"Diabetes Therapy","volume":" ","pages":"855-867"},"PeriodicalIF":4.2000,"publicationDate":"2024-04-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10951167/pdf/","citationCount":"0","resultStr":"{\"title\":\"Glycemic and Cost Outcomes among Hispanic/Latino People with Type 2 Diabetes in the USA Initiating Dulaglutide versus Basal Insulin: a Real-World Study.\",\"authors\":\"Meredith Hoog, Juan M Maldonado, Ruth Wangia-Dixon, Rachel Halpern, Erin Buysman, Garrett W Gremel, Ahong Huang, Manige Konig\",\"doi\":\"10.1007/s13300-024-01542-5\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Introduction: </strong>Optimal glycemic management after diabetes onset remains a challenge in Hispanic/Latino adults with type 2 diabetes (T2D), often resulting in poor health outcomes and higher rates of diabetes-related complications. The aim of this study was to examine and compare demographic and clinical characteristics, glycemic outcomes, health care resource utilization (HCRU), and costs among injection-naïve Hispanic/Latino adults with T2D initiating dulaglutide or basal insulin.</p><p><strong>Methods: </strong>This retrospective, observational study used administrative claims data from the Optum Research Database. Hispanic/Latino adults with T2D were assigned to dulaglutide or basal insulin cohorts on the basis of pharmacy claims and were propensity-score matched on demographic and baseline characteristics. Measures of glycemic management included 12 month follow-up glycated hemoglobin (HbA1c) and change in HbA1c from baseline. Follow-up all-cause and diabetes-related HCRU and costs, including costs per 1% change in HbA1c, were compared between cohorts.</p><p><strong>Results: </strong>The final propensity-score matched sample included 2872 patients: 1436 patients in each cohort. Mean (SD) reduction in HbA1c from baseline to 12 month follow-up was greater in the dulaglutide cohort compared with the basal insulin cohort [-1.40% (1.88) versus -0.92% (2.07); p < 0.001]. The dulaglutide cohort had significantly lower proportions of patients with ≥ 1 all-cause and diabetes-related outpatient visits, emergency room visits, and inpatient stays compared with the basal insulin cohort (p < 0.05). The dulaglutide cohort had significantly lower all-cause total costs per 1% HbA1c reduction than the basal insulin cohort ($13,768 versus $19,128; p < 0.001). Diabetes-related costs per 1% reduction were numerically lower for the dulaglutide cohort, but the difference was not statistically significant ($9737 versus $11,403; p = 0.081).</p><p><strong>Conclusions: </strong>Dulaglutide demonstrated better glycemic outcomes and lower all-cause costs per 1% HbA1c reduction among Hispanic/Latino adults compared with those initiating basal insulin. Our real-world findings in the Hispanic/Latino population were consistent with results obtained from the overall population and confirm the glycemic benefits of dulaglutide observed in clinical settings.</p>\",\"PeriodicalId\":11192,\"journal\":{\"name\":\"Diabetes Therapy\",\"volume\":\" \",\"pages\":\"855-867\"},\"PeriodicalIF\":4.2000,\"publicationDate\":\"2024-04-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10951167/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Diabetes Therapy\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1007/s13300-024-01542-5\",\"RegionNum\":3,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2024/3/1 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q2\",\"JCRName\":\"Medicine\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Diabetes Therapy","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1007/s13300-024-01542-5","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/3/1 0:00:00","PubModel":"Epub","JCR":"Q2","JCRName":"Medicine","Score":null,"Total":0}
Glycemic and Cost Outcomes among Hispanic/Latino People with Type 2 Diabetes in the USA Initiating Dulaglutide versus Basal Insulin: a Real-World Study.
Introduction: Optimal glycemic management after diabetes onset remains a challenge in Hispanic/Latino adults with type 2 diabetes (T2D), often resulting in poor health outcomes and higher rates of diabetes-related complications. The aim of this study was to examine and compare demographic and clinical characteristics, glycemic outcomes, health care resource utilization (HCRU), and costs among injection-naïve Hispanic/Latino adults with T2D initiating dulaglutide or basal insulin.
Methods: This retrospective, observational study used administrative claims data from the Optum Research Database. Hispanic/Latino adults with T2D were assigned to dulaglutide or basal insulin cohorts on the basis of pharmacy claims and were propensity-score matched on demographic and baseline characteristics. Measures of glycemic management included 12 month follow-up glycated hemoglobin (HbA1c) and change in HbA1c from baseline. Follow-up all-cause and diabetes-related HCRU and costs, including costs per 1% change in HbA1c, were compared between cohorts.
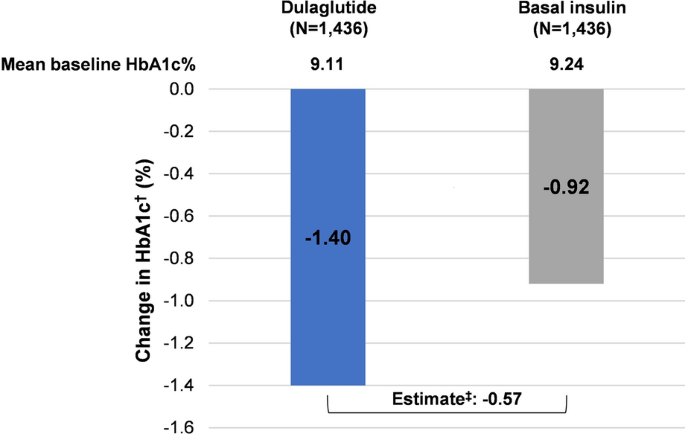
Results: The final propensity-score matched sample included 2872 patients: 1436 patients in each cohort. Mean (SD) reduction in HbA1c from baseline to 12 month follow-up was greater in the dulaglutide cohort compared with the basal insulin cohort [-1.40% (1.88) versus -0.92% (2.07); p < 0.001]. The dulaglutide cohort had significantly lower proportions of patients with ≥ 1 all-cause and diabetes-related outpatient visits, emergency room visits, and inpatient stays compared with the basal insulin cohort (p < 0.05). The dulaglutide cohort had significantly lower all-cause total costs per 1% HbA1c reduction than the basal insulin cohort ($13,768 versus $19,128; p < 0.001). Diabetes-related costs per 1% reduction were numerically lower for the dulaglutide cohort, but the difference was not statistically significant ($9737 versus $11,403; p = 0.081).
Conclusions: Dulaglutide demonstrated better glycemic outcomes and lower all-cause costs per 1% HbA1c reduction among Hispanic/Latino adults compared with those initiating basal insulin. Our real-world findings in the Hispanic/Latino population were consistent with results obtained from the overall population and confirm the glycemic benefits of dulaglutide observed in clinical settings.
期刊介绍:
Diabetes Therapy is an international, peer reviewed, rapid-publication (peer review in 2 weeks, published 3–4 weeks from acceptance) journal dedicated to the publication of high-quality clinical (all phases), observational, real-world, and health outcomes research around the discovery, development, and use of therapeutics and interventions (including devices) across all areas of diabetes. Studies relating to diagnostics and diagnosis, pharmacoeconomics, public health, epidemiology, quality of life, and patient care, management, and education are also encouraged.
The journal is of interest to a broad audience of healthcare professionals and publishes original research, reviews, communications and letters. The journal is read by a global audience and receives submissions from all over the world. Diabetes Therapy will consider all scientifically sound research be it positive, confirmatory or negative data. Submissions are welcomed whether they relate to an international and/or a country-specific audience, something that is crucially important when researchers are trying to target more specific patient populations. This inclusive approach allows the journal to assist in the dissemination of all scientifically and ethically sound research.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
