Ahmed Hassan, Kalaiyarasi Arujunan, Ali Mohamed, Vickey Katheria, Kevin Ashton, Rami Ahmed, Daren Subar
{"title":"结直肠肝转移肝脏手术后切口疝的发生率。腹腔镜手术能降低风险吗?一项比较研究。","authors":"Ahmed Hassan, Kalaiyarasi Arujunan, Ali Mohamed, Vickey Katheria, Kevin Ashton, Rami Ahmed, Daren Subar","doi":"10.14701/ahbps.23-138","DOIUrl":null,"url":null,"abstract":"<p><strong>Backgrounds/aims: </strong>No reports to compare incisional hernia (IH) incidence between laparoscopic and open colorectal liver metastases (CRLM) resections have previously been made. This is the first comparative study.</p><p><strong>Methods: </strong>Single-center retrospective review of patients who underwent CRLM surgery between January 2011 and December 2018. IH relating to liver surgery was confirmed by computed tomography. Patients were divided into laparoscopic liver resection (LLR) and open liver resection (OLR) groups. Data collection included age, sex, presence of diabetes mellitus, steroid intake, history of previous hernia or liver resection, subcutaneous and peri-renal fat thickness, preoperative creatinine and albumin, American Society of Anesthesiologists (ASA) score, major liver resection, surgical site infection, synchronous presentation, and preoperative chemotherapy.</p><p><strong>Results: </strong>Two hundred and forty-seven patients were included with a mean follow-up period of 41 ± 29 months (mean ± standard deviation). Eighty seven (35%) patients had LLR and 160 patients had OLR. No significant difference in the incidence of IH between LLR and OLR was found at 1 and 3 years, respectively ([10%, 19%] vs. [10%, 19%], <i>p</i> = 0.95). On multivariate analysis, previous hernia history (hazard ratio [HR], 2.22; 95% confidence interval [CI], 1.56-4.86) and subcutaneous fat thickness (HR, 2.22; 95% CI, 1.19-4.13) were independent risk factors. Length of hospital stay was shorter in LLR (6 ± 4 days vs. 10 ± 8 days, <i>p</i> < 0.001), in comparison to OLR.</p><p><strong>Conclusions: </strong>In CRLM, no difference in the incidence of IH between LLR and OLR was found. Previous hernia and subcutaneous fat thickness were risk factors. Further studies are needed to assess modifiable risk factors to develop IH in LLR.</p>","PeriodicalId":72220,"journal":{"name":"Annals of hepato-biliary-pancreatic surgery","volume":" ","pages":"155-160"},"PeriodicalIF":1.7000,"publicationDate":"2024-05-31","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11128795/pdf/","citationCount":"0","resultStr":"{\"title\":\"Incidence of incisional hernia following liver surgery for colorectal liver metastases. Does the laparoscopic approach reduce the risk? A comparative study.\",\"authors\":\"Ahmed Hassan, Kalaiyarasi Arujunan, Ali Mohamed, Vickey Katheria, Kevin Ashton, Rami Ahmed, Daren Subar\",\"doi\":\"10.14701/ahbps.23-138\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Backgrounds/aims: </strong>No reports to compare incisional hernia (IH) incidence between laparoscopic and open colorectal liver metastases (CRLM) resections have previously been made. This is the first comparative study.</p><p><strong>Methods: </strong>Single-center retrospective review of patients who underwent CRLM surgery between January 2011 and December 2018. IH relating to liver surgery was confirmed by computed tomography. Patients were divided into laparoscopic liver resection (LLR) and open liver resection (OLR) groups. Data collection included age, sex, presence of diabetes mellitus, steroid intake, history of previous hernia or liver resection, subcutaneous and peri-renal fat thickness, preoperative creatinine and albumin, American Society of Anesthesiologists (ASA) score, major liver resection, surgical site infection, synchronous presentation, and preoperative chemotherapy.</p><p><strong>Results: </strong>Two hundred and forty-seven patients were included with a mean follow-up period of 41 ± 29 months (mean ± standard deviation). Eighty seven (35%) patients had LLR and 160 patients had OLR. No significant difference in the incidence of IH between LLR and OLR was found at 1 and 3 years, respectively ([10%, 19%] vs. [10%, 19%], <i>p</i> = 0.95). On multivariate analysis, previous hernia history (hazard ratio [HR], 2.22; 95% confidence interval [CI], 1.56-4.86) and subcutaneous fat thickness (HR, 2.22; 95% CI, 1.19-4.13) were independent risk factors. Length of hospital stay was shorter in LLR (6 ± 4 days vs. 10 ± 8 days, <i>p</i> < 0.001), in comparison to OLR.</p><p><strong>Conclusions: </strong>In CRLM, no difference in the incidence of IH between LLR and OLR was found. Previous hernia and subcutaneous fat thickness were risk factors. Further studies are needed to assess modifiable risk factors to develop IH in LLR.</p>\",\"PeriodicalId\":72220,\"journal\":{\"name\":\"Annals of hepato-biliary-pancreatic surgery\",\"volume\":\" \",\"pages\":\"155-160\"},\"PeriodicalIF\":1.7000,\"publicationDate\":\"2024-05-31\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11128795/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Annals of hepato-biliary-pancreatic surgery\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.14701/ahbps.23-138\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2024/3/4 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q4\",\"JCRName\":\"GASTROENTEROLOGY & HEPATOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Annals of hepato-biliary-pancreatic surgery","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.14701/ahbps.23-138","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/3/4 0:00:00","PubModel":"Epub","JCR":"Q4","JCRName":"GASTROENTEROLOGY & HEPATOLOGY","Score":null,"Total":0}
Incidence of incisional hernia following liver surgery for colorectal liver metastases. Does the laparoscopic approach reduce the risk? A comparative study.
Backgrounds/aims: No reports to compare incisional hernia (IH) incidence between laparoscopic and open colorectal liver metastases (CRLM) resections have previously been made. This is the first comparative study.
Methods: Single-center retrospective review of patients who underwent CRLM surgery between January 2011 and December 2018. IH relating to liver surgery was confirmed by computed tomography. Patients were divided into laparoscopic liver resection (LLR) and open liver resection (OLR) groups. Data collection included age, sex, presence of diabetes mellitus, steroid intake, history of previous hernia or liver resection, subcutaneous and peri-renal fat thickness, preoperative creatinine and albumin, American Society of Anesthesiologists (ASA) score, major liver resection, surgical site infection, synchronous presentation, and preoperative chemotherapy.
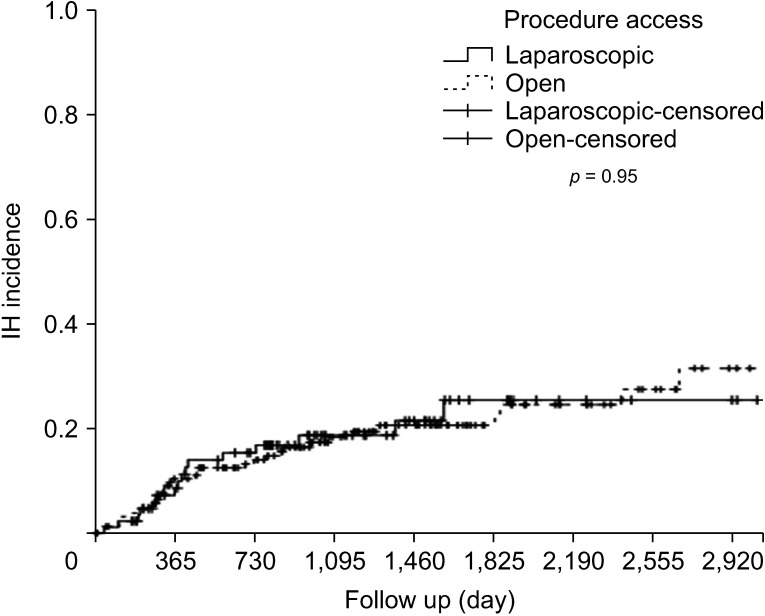
Results: Two hundred and forty-seven patients were included with a mean follow-up period of 41 ± 29 months (mean ± standard deviation). Eighty seven (35%) patients had LLR and 160 patients had OLR. No significant difference in the incidence of IH between LLR and OLR was found at 1 and 3 years, respectively ([10%, 19%] vs. [10%, 19%], p = 0.95). On multivariate analysis, previous hernia history (hazard ratio [HR], 2.22; 95% confidence interval [CI], 1.56-4.86) and subcutaneous fat thickness (HR, 2.22; 95% CI, 1.19-4.13) were independent risk factors. Length of hospital stay was shorter in LLR (6 ± 4 days vs. 10 ± 8 days, p < 0.001), in comparison to OLR.
Conclusions: In CRLM, no difference in the incidence of IH between LLR and OLR was found. Previous hernia and subcutaneous fat thickness were risk factors. Further studies are needed to assess modifiable risk factors to develop IH in LLR.


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
