James W. Schurr, Lara Ambrosi, Jillian Fitzgerald, Christian Bermudez, Michael V. Genuardi, Mark Brahier, Tonya Elliot, Kevin McGowan, Akram Zaaqoq, Sonjoy Laskar, Stuart M. Pope, Michael M. Givertz, Hari Mallidi, Katelyn W. Sylvester, Frank C. Seifert, Allison J. McLarty
{"title":"多中心评估心源性休克患者植入左心室辅助装置与否的 ECMO 桥接。","authors":"James W. Schurr, Lara Ambrosi, Jillian Fitzgerald, Christian Bermudez, Michael V. Genuardi, Mark Brahier, Tonya Elliot, Kevin McGowan, Akram Zaaqoq, Sonjoy Laskar, Stuart M. Pope, Michael M. Givertz, Hari Mallidi, Katelyn W. Sylvester, Frank C. Seifert, Allison J. McLarty","doi":"10.1111/aor.14740","DOIUrl":null,"url":null,"abstract":"<div>\n \n \n <section>\n \n <h3> Background</h3>\n \n <p>The efficacy of extracorporeal membrane oxygenation (ECMO) as a bridge to left ventricular assist device (LVAD) remains unclear, and recipients of the more contemporary HeartMate 3 (HM3) LVAD are not well represented in previous studies. We therefore undertook a multicenter, retrospective study of this population.</p>\n </section>\n \n <section>\n \n <h3> Methods and Results</h3>\n \n <p>INTERMACS 1 LVAD recipients from five U.S. centers were included. In-hospital and one-year outcomes were recorded. The primary outcome was the overall mortality hazard comparing ECMO versus non-ECMO patients by propensity-weighted survival analysis. Secondary outcomes included survival by LVAD type, as well as postoperative and one-year outcomes. One hundred and twenty-seven patients were included; 24 received ECMO as a bridge to LVAD. Mortality was higher in patients bridged with ECMO in the primary analysis (HR 3.22 [95%CI 1.06–9.77], <i>p</i> = 0.039). Right ventricular assist device was more common in the ECMO group (ECMO: 54.2% vs non-ECMO: 11.7%, <i>p</i> < 0.001). Ischemic stroke was higher at one year in the ECMO group (ECMO: 25.0% vs non-ECMO: 4.9%, <i>p</i> = 0.006). Among the study cohort, one-year mortality was lower in HM3 than in HeartMate II (HMII) or HeartWare HVAD (10.5% vs 46.9% vs 31.6%, respectively; <i>p</i> < 0.001) recipients. Pump thrombosis at one year was lower in HM3 than in HMII or HVAD (1.8% vs 16.1% vs 16.2%, respectively; <i>p</i> = 0.026) recipients.</p>\n </section>\n \n <section>\n \n <h3> Conclusions</h3>\n \n <p>Higher mortality was observed with ECMO as a bridge to LVAD, likely due to higher acuity illness, yet acceptable one-year survival was seen compared with historical rates. The receipt of the HM3 was associated with improved survival compared with older generation devices.</p>\n </section>\n </div>","PeriodicalId":8450,"journal":{"name":"Artificial organs","volume":"48 8","pages":"921-931"},"PeriodicalIF":2.3000,"publicationDate":"2024-03-08","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1111/aor.14740","citationCount":"0","resultStr":"{\"title\":\"Multicenter evaluation of left ventricular assist device implantation with or without ECMO bridge in cardiogenic shock\",\"authors\":\"James W. Schurr, Lara Ambrosi, Jillian Fitzgerald, Christian Bermudez, Michael V. Genuardi, Mark Brahier, Tonya Elliot, Kevin McGowan, Akram Zaaqoq, Sonjoy Laskar, Stuart M. Pope, Michael M. Givertz, Hari Mallidi, Katelyn W. Sylvester, Frank C. Seifert, Allison J. McLarty\",\"doi\":\"10.1111/aor.14740\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<div>\\n \\n \\n <section>\\n \\n <h3> Background</h3>\\n \\n <p>The efficacy of extracorporeal membrane oxygenation (ECMO) as a bridge to left ventricular assist device (LVAD) remains unclear, and recipients of the more contemporary HeartMate 3 (HM3) LVAD are not well represented in previous studies. We therefore undertook a multicenter, retrospective study of this population.</p>\\n </section>\\n \\n <section>\\n \\n <h3> Methods and Results</h3>\\n \\n <p>INTERMACS 1 LVAD recipients from five U.S. centers were included. In-hospital and one-year outcomes were recorded. The primary outcome was the overall mortality hazard comparing ECMO versus non-ECMO patients by propensity-weighted survival analysis. Secondary outcomes included survival by LVAD type, as well as postoperative and one-year outcomes. One hundred and twenty-seven patients were included; 24 received ECMO as a bridge to LVAD. Mortality was higher in patients bridged with ECMO in the primary analysis (HR 3.22 [95%CI 1.06–9.77], <i>p</i> = 0.039). Right ventricular assist device was more common in the ECMO group (ECMO: 54.2% vs non-ECMO: 11.7%, <i>p</i> < 0.001). Ischemic stroke was higher at one year in the ECMO group (ECMO: 25.0% vs non-ECMO: 4.9%, <i>p</i> = 0.006). Among the study cohort, one-year mortality was lower in HM3 than in HeartMate II (HMII) or HeartWare HVAD (10.5% vs 46.9% vs 31.6%, respectively; <i>p</i> < 0.001) recipients. Pump thrombosis at one year was lower in HM3 than in HMII or HVAD (1.8% vs 16.1% vs 16.2%, respectively; <i>p</i> = 0.026) recipients.</p>\\n </section>\\n \\n <section>\\n \\n <h3> Conclusions</h3>\\n \\n <p>Higher mortality was observed with ECMO as a bridge to LVAD, likely due to higher acuity illness, yet acceptable one-year survival was seen compared with historical rates. The receipt of the HM3 was associated with improved survival compared with older generation devices.</p>\\n </section>\\n </div>\",\"PeriodicalId\":8450,\"journal\":{\"name\":\"Artificial organs\",\"volume\":\"48 8\",\"pages\":\"921-931\"},\"PeriodicalIF\":2.3000,\"publicationDate\":\"2024-03-08\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://onlinelibrary.wiley.com/doi/epdf/10.1111/aor.14740\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Artificial organs\",\"FirstCategoryId\":\"5\",\"ListUrlMain\":\"https://onlinelibrary.wiley.com/doi/10.1111/aor.14740\",\"RegionNum\":3,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q3\",\"JCRName\":\"ENGINEERING, BIOMEDICAL\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Artificial organs","FirstCategoryId":"5","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1111/aor.14740","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"ENGINEERING, BIOMEDICAL","Score":null,"Total":0}
Multicenter evaluation of left ventricular assist device implantation with or without ECMO bridge in cardiogenic shock
Background
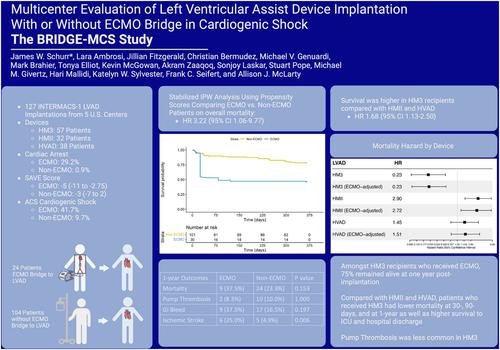
The efficacy of extracorporeal membrane oxygenation (ECMO) as a bridge to left ventricular assist device (LVAD) remains unclear, and recipients of the more contemporary HeartMate 3 (HM3) LVAD are not well represented in previous studies. We therefore undertook a multicenter, retrospective study of this population.
Methods and Results
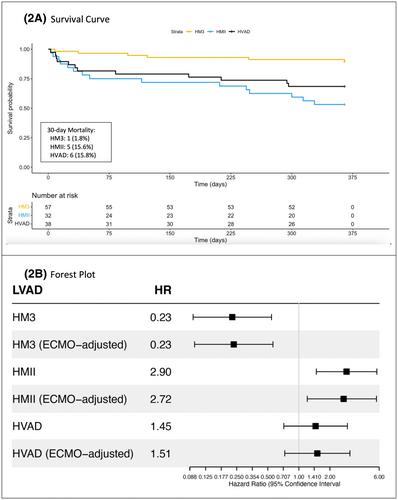
INTERMACS 1 LVAD recipients from five U.S. centers were included. In-hospital and one-year outcomes were recorded. The primary outcome was the overall mortality hazard comparing ECMO versus non-ECMO patients by propensity-weighted survival analysis. Secondary outcomes included survival by LVAD type, as well as postoperative and one-year outcomes. One hundred and twenty-seven patients were included; 24 received ECMO as a bridge to LVAD. Mortality was higher in patients bridged with ECMO in the primary analysis (HR 3.22 [95%CI 1.06–9.77], p = 0.039). Right ventricular assist device was more common in the ECMO group (ECMO: 54.2% vs non-ECMO: 11.7%, p < 0.001). Ischemic stroke was higher at one year in the ECMO group (ECMO: 25.0% vs non-ECMO: 4.9%, p = 0.006). Among the study cohort, one-year mortality was lower in HM3 than in HeartMate II (HMII) or HeartWare HVAD (10.5% vs 46.9% vs 31.6%, respectively; p < 0.001) recipients. Pump thrombosis at one year was lower in HM3 than in HMII or HVAD (1.8% vs 16.1% vs 16.2%, respectively; p = 0.026) recipients.
Conclusions
Higher mortality was observed with ECMO as a bridge to LVAD, likely due to higher acuity illness, yet acceptable one-year survival was seen compared with historical rates. The receipt of the HM3 was associated with improved survival compared with older generation devices.
期刊介绍:
Artificial Organs is the official peer reviewed journal of The International Federation for Artificial Organs (Members of the Federation are: The American Society for Artificial Internal Organs, The European Society for Artificial Organs, and The Japanese Society for Artificial Organs), The International Faculty for Artificial Organs, the International Society for Rotary Blood Pumps, The International Society for Pediatric Mechanical Cardiopulmonary Support, and the Vienna International Workshop on Functional Electrical Stimulation. Artificial Organs publishes original research articles dealing with developments in artificial organs applications and treatment modalities and their clinical applications worldwide. Membership in the Societies listed above is not a prerequisite for publication. Articles are published without charge to the author except for color figures and excess page charges as noted.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
