{"title":"氯胺酮对重症患者预后的影响:随机对照试验的荟萃分析和试验序列分析系统综述。","authors":"Yerkin Abdildin, Karina Tapinova, Assel Nemerenova, Dmitriy Viderman","doi":"10.4266/acc.2023.00829","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>This meta-analysis aims to evaluate the effects of ketamine in critically ill intensive care unit (ICU) patients.</p><p><strong>Methods: </strong>We searched for randomized controlled trials (RCTs) in PubMed, Scopus, and the Cochrane Library; the search was performed initially in January but was repeated in December of 2023. We focused on ICU patients of any age. We included studies that compared ketamine with other traditional agents used in the ICU. We synthesized evidence using RevMan v5.4 and presented the results as forest plots. We also used trial sequential analysis (TSA) software v. 0.9.5.10 Beta and presented results as TSA plots. For synthesizing results, we used a random-effects model and reported differences in outcomes of two groups in terms of mean difference (MD), standardized MD, and risk ratio with 95% confidence interval. We assessed the risk of bias using the Cochrane RoB tool for RCTs. Our outcomes were mortality, pain, opioid and midazolam requirements, delirium rates, and ICU length of stay.</p><p><strong>Results: </strong>Twelve RCTs involving 805 ICU patients (ketamine group, n=398; control group, n=407) were included in the meta-analysis. The ketamine group was not superior to the control group in terms of mortality (in five studies with 318 patients), pain (two studies with 129 patients), mean and cumulative opioid consumption (six studies with 494 patients), midazolam consumption (six studies with 304 patients), and ICU length of stay (three studies with 270 patients). However, the model favored the ketamine group over the control group in delirium rate (four studies with 358 patients). This result is significant in terms of conventional boundaries (alpha=5%) but is not robust in sequential analysis. The applicability of the findings is limited by the small number of patients pooled for each outcome.</p><p><strong>Conclusions: </strong>Our meta-analysis did not demonstrate differences between ketamine and control groups regarding any outcome except delirium rate, where the model favored the ketamine group over the control group. However, this result is not robust as sensitivity analysis and trial sequential analysis suggest that more RCTs should be conducted in the future.</p>","PeriodicalId":44118,"journal":{"name":"Acute and Critical Care","volume":"39 1","pages":"34-46"},"PeriodicalIF":2.0000,"publicationDate":"2024-02-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11002615/pdf/","citationCount":"0","resultStr":"{\"title\":\"The impact of ketamine on outcomes in critically ill patients: a systematic review with meta-analysis and trial sequential analysis of randomized controlled trials.\",\"authors\":\"Yerkin Abdildin, Karina Tapinova, Assel Nemerenova, Dmitriy Viderman\",\"doi\":\"10.4266/acc.2023.00829\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>This meta-analysis aims to evaluate the effects of ketamine in critically ill intensive care unit (ICU) patients.</p><p><strong>Methods: </strong>We searched for randomized controlled trials (RCTs) in PubMed, Scopus, and the Cochrane Library; the search was performed initially in January but was repeated in December of 2023. We focused on ICU patients of any age. We included studies that compared ketamine with other traditional agents used in the ICU. We synthesized evidence using RevMan v5.4 and presented the results as forest plots. We also used trial sequential analysis (TSA) software v. 0.9.5.10 Beta and presented results as TSA plots. For synthesizing results, we used a random-effects model and reported differences in outcomes of two groups in terms of mean difference (MD), standardized MD, and risk ratio with 95% confidence interval. We assessed the risk of bias using the Cochrane RoB tool for RCTs. Our outcomes were mortality, pain, opioid and midazolam requirements, delirium rates, and ICU length of stay.</p><p><strong>Results: </strong>Twelve RCTs involving 805 ICU patients (ketamine group, n=398; control group, n=407) were included in the meta-analysis. The ketamine group was not superior to the control group in terms of mortality (in five studies with 318 patients), pain (two studies with 129 patients), mean and cumulative opioid consumption (six studies with 494 patients), midazolam consumption (six studies with 304 patients), and ICU length of stay (three studies with 270 patients). However, the model favored the ketamine group over the control group in delirium rate (four studies with 358 patients). This result is significant in terms of conventional boundaries (alpha=5%) but is not robust in sequential analysis. The applicability of the findings is limited by the small number of patients pooled for each outcome.</p><p><strong>Conclusions: </strong>Our meta-analysis did not demonstrate differences between ketamine and control groups regarding any outcome except delirium rate, where the model favored the ketamine group over the control group. However, this result is not robust as sensitivity analysis and trial sequential analysis suggest that more RCTs should be conducted in the future.</p>\",\"PeriodicalId\":44118,\"journal\":{\"name\":\"Acute and Critical Care\",\"volume\":\"39 1\",\"pages\":\"34-46\"},\"PeriodicalIF\":2.0000,\"publicationDate\":\"2024-02-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11002615/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Acute and Critical Care\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.4266/acc.2023.00829\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2024/2/28 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q3\",\"JCRName\":\"CRITICAL CARE MEDICINE\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Acute and Critical Care","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.4266/acc.2023.00829","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/2/28 0:00:00","PubModel":"Epub","JCR":"Q3","JCRName":"CRITICAL CARE MEDICINE","Score":null,"Total":0}
The impact of ketamine on outcomes in critically ill patients: a systematic review with meta-analysis and trial sequential analysis of randomized controlled trials.
Background: This meta-analysis aims to evaluate the effects of ketamine in critically ill intensive care unit (ICU) patients.
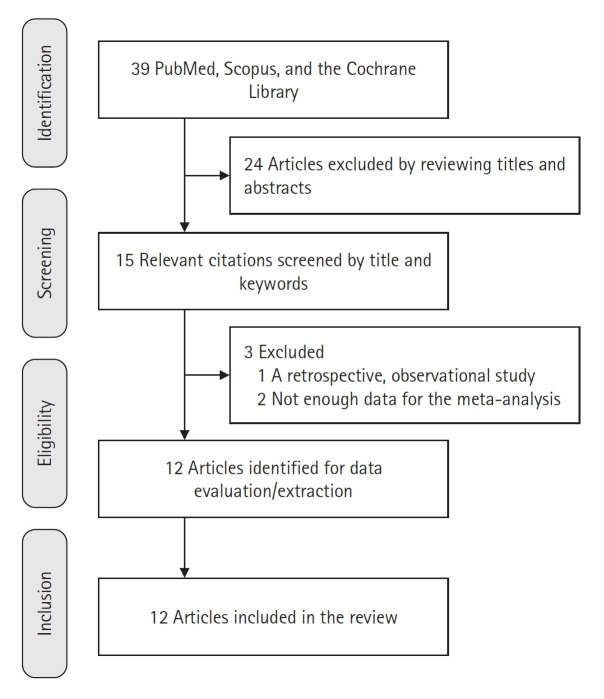
Methods: We searched for randomized controlled trials (RCTs) in PubMed, Scopus, and the Cochrane Library; the search was performed initially in January but was repeated in December of 2023. We focused on ICU patients of any age. We included studies that compared ketamine with other traditional agents used in the ICU. We synthesized evidence using RevMan v5.4 and presented the results as forest plots. We also used trial sequential analysis (TSA) software v. 0.9.5.10 Beta and presented results as TSA plots. For synthesizing results, we used a random-effects model and reported differences in outcomes of two groups in terms of mean difference (MD), standardized MD, and risk ratio with 95% confidence interval. We assessed the risk of bias using the Cochrane RoB tool for RCTs. Our outcomes were mortality, pain, opioid and midazolam requirements, delirium rates, and ICU length of stay.
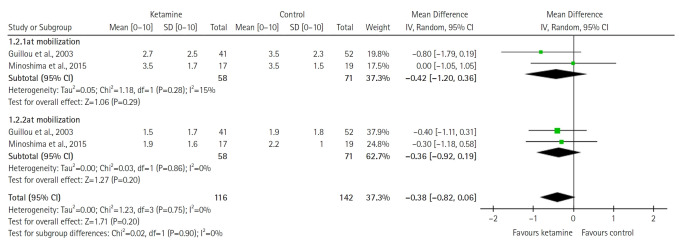
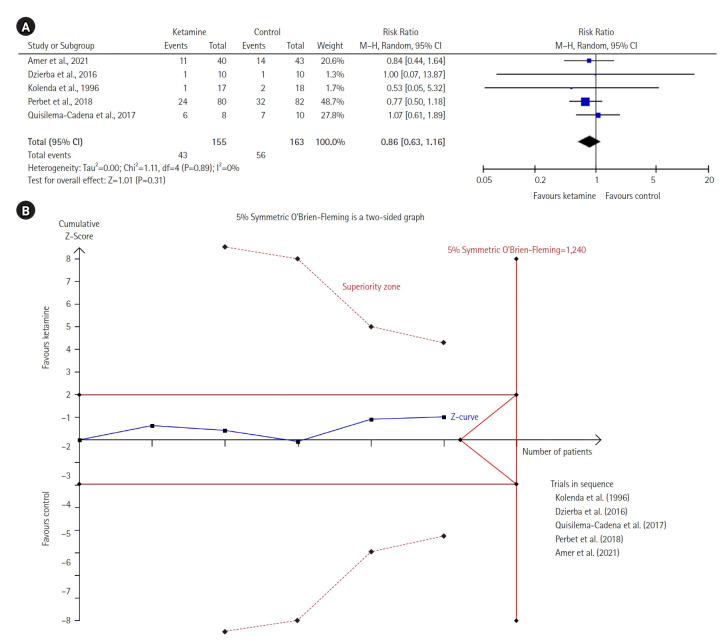
Results: Twelve RCTs involving 805 ICU patients (ketamine group, n=398; control group, n=407) were included in the meta-analysis. The ketamine group was not superior to the control group in terms of mortality (in five studies with 318 patients), pain (two studies with 129 patients), mean and cumulative opioid consumption (six studies with 494 patients), midazolam consumption (six studies with 304 patients), and ICU length of stay (three studies with 270 patients). However, the model favored the ketamine group over the control group in delirium rate (four studies with 358 patients). This result is significant in terms of conventional boundaries (alpha=5%) but is not robust in sequential analysis. The applicability of the findings is limited by the small number of patients pooled for each outcome.
Conclusions: Our meta-analysis did not demonstrate differences between ketamine and control groups regarding any outcome except delirium rate, where the model favored the ketamine group over the control group. However, this result is not robust as sensitivity analysis and trial sequential analysis suggest that more RCTs should be conducted in the future.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
