Marielen Reinhardt, Tobias Schupp, Mohammad Abumayyaleh, Felix Lau, Alexander Schmitt, Noah Abel, Muharrem Akin, Jonas Rusnak, Ibrahim Akin, Michael Behnes
{"title":"射血分数轻度降低的心力衰竭患者的肥胖悖论","authors":"Marielen Reinhardt, Tobias Schupp, Mohammad Abumayyaleh, Felix Lau, Alexander Schmitt, Noah Abel, Muharrem Akin, Jonas Rusnak, Ibrahim Akin, Michael Behnes","doi":"10.2147/POR.S444361","DOIUrl":null,"url":null,"abstract":"<p><strong>Objective: </strong>The study investigates the prognostic impact of body mass index (BMI) in patients hospitalized with heart failure with mildly reduced ejection fraction (HFmrEF).</p><p><strong>Background: </strong>Limited data regarding the prognostic impact of BMI in patients with HFmrEF is available.</p><p><strong>Methods: </strong>Consecutive patients with HFmrEF (ie, left ventricular ejection fraction 41-49% and signs and/or symptoms of HF) were retrospectively included at one institution from 2016 to 2022. Risk stratification was performed according to WHO-defined BMI groups. The primary endpoint was all-cause mortality at 30 months (median follow-up). Kaplan-Meier, uni- and multivariable Cox proportional regression analyses were applied for statistics.</p><p><strong>Results: </strong>1832 consecutive patients with HFmrEF were included with a median BMI of 26.7 kg/m<sup>2</sup> (IQR 24.0-30.8 kg/m<sup>2</sup>). Patients with lowest BMI (ie, 18.5-24.9 kg/m<sup>2</sup>) were associated with highest risk of all-cause mortality at 30 months compared to patients with higher BMI values (40.0% vs 29.0% vs 21.4% vs 20.9%; log rank p = 0.001; HR = 0.721; 95% CI 0.656-0.793; p = 0.001). Even after multivariable adjustment, higher BMI values were associated with improved survival at 30 months (HR = 0.963; 95% CI 0.943-0.985; p = 0.001). In contrast, the risk of HF- related rehospitalization at 30 months was not affected by BMI (log rank p = 0.064).</p><p><strong>Conclusion: </strong>In patients hospitalized with HFmrEF, lower BMI was associated with increased risk of all-cause mortality at 30 months, suggesting an obesity paradox in HFmrEF.</p>","PeriodicalId":20399,"journal":{"name":"Pragmatic and Observational Research","volume":"15 ","pages":"31-43"},"PeriodicalIF":2.7000,"publicationDate":"2024-03-05","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10933520/pdf/","citationCount":"0","resultStr":"{\"title\":\"Obesity Paradox in Heart Failure with Mildly Reduced Ejection Fraction.\",\"authors\":\"Marielen Reinhardt, Tobias Schupp, Mohammad Abumayyaleh, Felix Lau, Alexander Schmitt, Noah Abel, Muharrem Akin, Jonas Rusnak, Ibrahim Akin, Michael Behnes\",\"doi\":\"10.2147/POR.S444361\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Objective: </strong>The study investigates the prognostic impact of body mass index (BMI) in patients hospitalized with heart failure with mildly reduced ejection fraction (HFmrEF).</p><p><strong>Background: </strong>Limited data regarding the prognostic impact of BMI in patients with HFmrEF is available.</p><p><strong>Methods: </strong>Consecutive patients with HFmrEF (ie, left ventricular ejection fraction 41-49% and signs and/or symptoms of HF) were retrospectively included at one institution from 2016 to 2022. Risk stratification was performed according to WHO-defined BMI groups. The primary endpoint was all-cause mortality at 30 months (median follow-up). Kaplan-Meier, uni- and multivariable Cox proportional regression analyses were applied for statistics.</p><p><strong>Results: </strong>1832 consecutive patients with HFmrEF were included with a median BMI of 26.7 kg/m<sup>2</sup> (IQR 24.0-30.8 kg/m<sup>2</sup>). Patients with lowest BMI (ie, 18.5-24.9 kg/m<sup>2</sup>) were associated with highest risk of all-cause mortality at 30 months compared to patients with higher BMI values (40.0% vs 29.0% vs 21.4% vs 20.9%; log rank p = 0.001; HR = 0.721; 95% CI 0.656-0.793; p = 0.001). Even after multivariable adjustment, higher BMI values were associated with improved survival at 30 months (HR = 0.963; 95% CI 0.943-0.985; p = 0.001). In contrast, the risk of HF- related rehospitalization at 30 months was not affected by BMI (log rank p = 0.064).</p><p><strong>Conclusion: </strong>In patients hospitalized with HFmrEF, lower BMI was associated with increased risk of all-cause mortality at 30 months, suggesting an obesity paradox in HFmrEF.</p>\",\"PeriodicalId\":20399,\"journal\":{\"name\":\"Pragmatic and Observational Research\",\"volume\":\"15 \",\"pages\":\"31-43\"},\"PeriodicalIF\":2.7000,\"publicationDate\":\"2024-03-05\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10933520/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Pragmatic and Observational Research\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.2147/POR.S444361\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2024/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q2\",\"JCRName\":\"MEDICINE, GENERAL & INTERNAL\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Pragmatic and Observational Research","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.2147/POR.S444361","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/1/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"MEDICINE, GENERAL & INTERNAL","Score":null,"Total":0}
引用次数: 0
摘要
研究目的该研究调查了体重指数(BMI)对射血分数轻度降低的心力衰竭(HFmrEF)住院患者的预后影响:有关体重指数对射血分数轻度降低型心力衰竭患者预后影响的数据有限:方法:回顾性纳入2016年至2022年一家机构的连续HFmrEF患者(即左心室射血分数41%-49%且有HF体征和/或症状)。根据世卫组织定义的体重指数分组进行风险分层。主要终点是随访30个月(中位数)的全因死亡率。采用卡普兰-梅耶、单变量和多变量考克斯比例回归分析进行统计:共纳入 1832 名连续的 HFmrEF 患者,中位体重指数为 26.7 kg/m2(IQR 24.0-30.8 kg/m2)。与 BMI 值较高的患者相比,BMI 值最低的患者(即 18.5-24.9 kg/m2)在 30 个月内的全因死亡风险最高(40.0% vs 29.0% vs 21.4% vs 20.9%;对数秩 p = 0.001;HR = 0.721;95% CI 0.656-0.793; p = 0.001)。即使经过多变量调整,较高的 BMI 值也与 30 个月的生存率提高有关(HR = 0.963;95% CI 0.943-0.985;P = 0.001)。相比之下,30 个月后与心房颤动相关的再住院风险不受 BMI 的影响(对数秩 p = 0.064):结论:在HFmrEF住院患者中,较低的体重指数与30个月后全因死亡风险增加有关,这表明HFmrEF存在肥胖悖论。
Obesity Paradox in Heart Failure with Mildly Reduced Ejection Fraction.
Objective: The study investigates the prognostic impact of body mass index (BMI) in patients hospitalized with heart failure with mildly reduced ejection fraction (HFmrEF).
Background: Limited data regarding the prognostic impact of BMI in patients with HFmrEF is available.
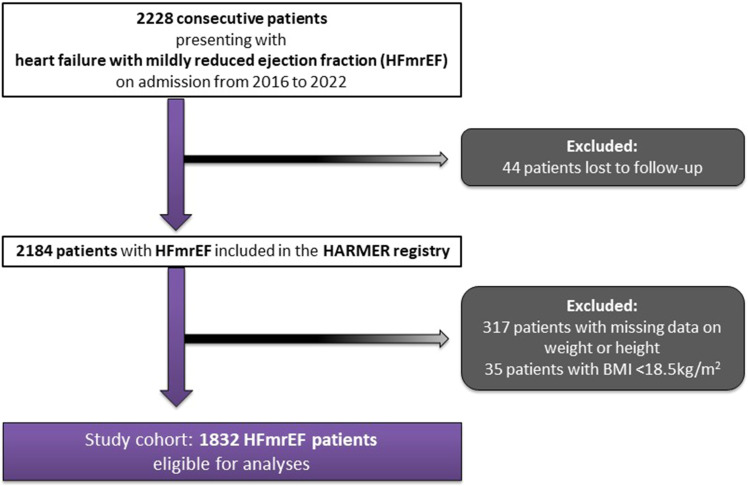
Methods: Consecutive patients with HFmrEF (ie, left ventricular ejection fraction 41-49% and signs and/or symptoms of HF) were retrospectively included at one institution from 2016 to 2022. Risk stratification was performed according to WHO-defined BMI groups. The primary endpoint was all-cause mortality at 30 months (median follow-up). Kaplan-Meier, uni- and multivariable Cox proportional regression analyses were applied for statistics.
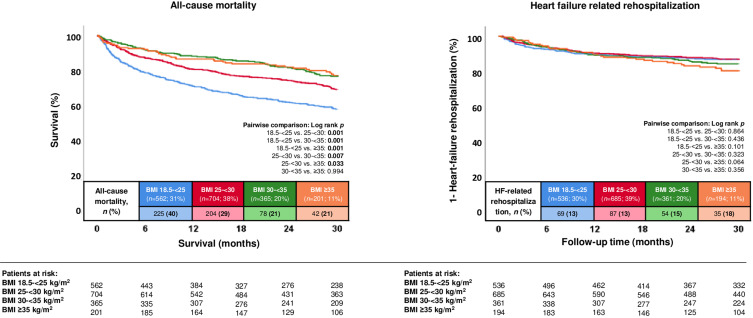
Results: 1832 consecutive patients with HFmrEF were included with a median BMI of 26.7 kg/m2 (IQR 24.0-30.8 kg/m2). Patients with lowest BMI (ie, 18.5-24.9 kg/m2) were associated with highest risk of all-cause mortality at 30 months compared to patients with higher BMI values (40.0% vs 29.0% vs 21.4% vs 20.9%; log rank p = 0.001; HR = 0.721; 95% CI 0.656-0.793; p = 0.001). Even after multivariable adjustment, higher BMI values were associated with improved survival at 30 months (HR = 0.963; 95% CI 0.943-0.985; p = 0.001). In contrast, the risk of HF- related rehospitalization at 30 months was not affected by BMI (log rank p = 0.064).
Conclusion: In patients hospitalized with HFmrEF, lower BMI was associated with increased risk of all-cause mortality at 30 months, suggesting an obesity paradox in HFmrEF.
期刊介绍:
Pragmatic and Observational Research is an international, peer-reviewed, open-access journal that publishes data from studies designed to closely reflect medical interventions in real-world clinical practice, providing insights beyond classical randomized controlled trials (RCTs). While RCTs maximize internal validity for cause-and-effect relationships, they often represent only specific patient groups. This journal aims to complement such studies by providing data that better mirrors real-world patients and the usage of medicines, thus informing guidelines and enhancing the applicability of research findings across diverse patient populations encountered in everyday clinical practice.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
