Jean-Pierre Tasu, Guillaume Herpe, Jérôme Damion, Jean-Pierre Richer, Bertrand Debeane, Mathilde Vionnet, Laetitia Rouleau, Michel Carretier, Aurélie Ferru, Pierre Ingrand, David Tougeron
{"title":"用不可逆电穿孔技术使最初无法切除的局部晚期胰腺癌接受手术治疗:IRECAP II 期研究。","authors":"Jean-Pierre Tasu, Guillaume Herpe, Jérôme Damion, Jean-Pierre Richer, Bertrand Debeane, Mathilde Vionnet, Laetitia Rouleau, Michel Carretier, Aurélie Ferru, Pierre Ingrand, David Tougeron","doi":"10.1007/s00330-024-10613-x","DOIUrl":null,"url":null,"abstract":"<p><strong>Objectives: </strong>The aim of the IRECAP study was to evaluate the rate of locally advanced pancreas cancer patients (LAPC) who could undergo R0 or R1 surgery after irreversible electroporation (IRE).</p><p><strong>Materials and methods: </strong>IRECAP study is a phase II, single-center, open-label, prospective, non-randomized trial registered at clinicaltrials.gov (NCT03105921). Patients with LAPC were first treated by 3-month neo-adjuvant chemotherapy in order to avoid inclusion of either patients with LAPC having become resectable after chemotherapy or patients with rapid disease progression. In cases of stable disease, IRE was performed percutaneously under CT guidance. Surgery was planned between 28 and 90 days after IRE. Tumor specimens were studied to evaluate the resection margins (R0/R1/R2).</p><p><strong>Results: </strong>Six men and 11 women were included (median age 61 years, range 37-77 years). No IRE-related death was observed. Ten patients (58%, 10/17) experienced 25 serious adverse events related to IRE. Four patients progressed between IRE and surgery and were excluded from surgery. Thirteen patients were finally operated, six withheld for pancreas resection, three for diffuse peritoneal carcinosis, two for massive vascular entrapment, and one for hepato-cellular carcinoma not diagnosed before surgery. Rate of R1-R0 was 35% (n = 6/17). Median overall survival was 31 months (95% CI; 4-undefined) for the six patients with R0/R1 resection and 21 months (95% CI; 4-25) for the 11 patients without resection or R2 resection (logrank p = 0.044).</p><p><strong>Conclusion: </strong>After neoadjuvant chemotherapy, IRE could provide R0 or R1 resection in 35% of LAPC, which seems to be associated with higher OS.</p><p><strong>Clinical relevance statement: </strong>After induction chemotherapy, stable locally advanced pancreatic cancers can be treated by irreversible electroporation, which could lead to a secondary 35% rate of R0 or R1 surgical resection which may be associated with a significantly higher overall survival.</p><p><strong>Key points: </strong>• In cases of unresectable LAPC (locally advanced pancreatic cancer), percutaneous irreversible electroporation (pIRE) is feasible (100% success rate of the procedure), but is associated with a 58% rate of grade 3-4 adverse events. • In patients with unresectable LAPC, pIRE could lead 35% of patients to R0-R1 surgical resection. • From IRE, median overall survival was 31 months (95% CI; 4-undefined) for the patients with R0/R1 resection and 21 months (95% CI; 4-25) for the patients without resection or R2 resection (logrank p = 0.044).</p>","PeriodicalId":12076,"journal":{"name":"European Radiology","volume":null,"pages":null},"PeriodicalIF":4.7000,"publicationDate":"2024-10-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"","citationCount":"0","resultStr":"{\"title\":\"Irreversible electroporation to bring initially unresectable locally advanced pancreatic adenocarcinoma to surgery: the IRECAP phase II study.\",\"authors\":\"Jean-Pierre Tasu, Guillaume Herpe, Jérôme Damion, Jean-Pierre Richer, Bertrand Debeane, Mathilde Vionnet, Laetitia Rouleau, Michel Carretier, Aurélie Ferru, Pierre Ingrand, David Tougeron\",\"doi\":\"10.1007/s00330-024-10613-x\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Objectives: </strong>The aim of the IRECAP study was to evaluate the rate of locally advanced pancreas cancer patients (LAPC) who could undergo R0 or R1 surgery after irreversible electroporation (IRE).</p><p><strong>Materials and methods: </strong>IRECAP study is a phase II, single-center, open-label, prospective, non-randomized trial registered at clinicaltrials.gov (NCT03105921). Patients with LAPC were first treated by 3-month neo-adjuvant chemotherapy in order to avoid inclusion of either patients with LAPC having become resectable after chemotherapy or patients with rapid disease progression. In cases of stable disease, IRE was performed percutaneously under CT guidance. Surgery was planned between 28 and 90 days after IRE. Tumor specimens were studied to evaluate the resection margins (R0/R1/R2).</p><p><strong>Results: </strong>Six men and 11 women were included (median age 61 years, range 37-77 years). No IRE-related death was observed. Ten patients (58%, 10/17) experienced 25 serious adverse events related to IRE. Four patients progressed between IRE and surgery and were excluded from surgery. Thirteen patients were finally operated, six withheld for pancreas resection, three for diffuse peritoneal carcinosis, two for massive vascular entrapment, and one for hepato-cellular carcinoma not diagnosed before surgery. Rate of R1-R0 was 35% (n = 6/17). Median overall survival was 31 months (95% CI; 4-undefined) for the six patients with R0/R1 resection and 21 months (95% CI; 4-25) for the 11 patients without resection or R2 resection (logrank p = 0.044).</p><p><strong>Conclusion: </strong>After neoadjuvant chemotherapy, IRE could provide R0 or R1 resection in 35% of LAPC, which seems to be associated with higher OS.</p><p><strong>Clinical relevance statement: </strong>After induction chemotherapy, stable locally advanced pancreatic cancers can be treated by irreversible electroporation, which could lead to a secondary 35% rate of R0 or R1 surgical resection which may be associated with a significantly higher overall survival.</p><p><strong>Key points: </strong>• In cases of unresectable LAPC (locally advanced pancreatic cancer), percutaneous irreversible electroporation (pIRE) is feasible (100% success rate of the procedure), but is associated with a 58% rate of grade 3-4 adverse events. • In patients with unresectable LAPC, pIRE could lead 35% of patients to R0-R1 surgical resection. • From IRE, median overall survival was 31 months (95% CI; 4-undefined) for the patients with R0/R1 resection and 21 months (95% CI; 4-25) for the patients without resection or R2 resection (logrank p = 0.044).</p>\",\"PeriodicalId\":12076,\"journal\":{\"name\":\"European Radiology\",\"volume\":null,\"pages\":null},\"PeriodicalIF\":4.7000,\"publicationDate\":\"2024-10-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"European Radiology\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1007/s00330-024-10613-x\",\"RegionNum\":2,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2024/3/18 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q1\",\"JCRName\":\"RADIOLOGY, NUCLEAR MEDICINE & MEDICAL IMAGING\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"European Radiology","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1007/s00330-024-10613-x","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/3/18 0:00:00","PubModel":"Epub","JCR":"Q1","JCRName":"RADIOLOGY, NUCLEAR MEDICINE & MEDICAL IMAGING","Score":null,"Total":0}
Irreversible electroporation to bring initially unresectable locally advanced pancreatic adenocarcinoma to surgery: the IRECAP phase II study.
Objectives: The aim of the IRECAP study was to evaluate the rate of locally advanced pancreas cancer patients (LAPC) who could undergo R0 or R1 surgery after irreversible electroporation (IRE).
Materials and methods: IRECAP study is a phase II, single-center, open-label, prospective, non-randomized trial registered at clinicaltrials.gov (NCT03105921). Patients with LAPC were first treated by 3-month neo-adjuvant chemotherapy in order to avoid inclusion of either patients with LAPC having become resectable after chemotherapy or patients with rapid disease progression. In cases of stable disease, IRE was performed percutaneously under CT guidance. Surgery was planned between 28 and 90 days after IRE. Tumor specimens were studied to evaluate the resection margins (R0/R1/R2).
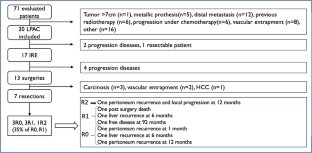
Results: Six men and 11 women were included (median age 61 years, range 37-77 years). No IRE-related death was observed. Ten patients (58%, 10/17) experienced 25 serious adverse events related to IRE. Four patients progressed between IRE and surgery and were excluded from surgery. Thirteen patients were finally operated, six withheld for pancreas resection, three for diffuse peritoneal carcinosis, two for massive vascular entrapment, and one for hepato-cellular carcinoma not diagnosed before surgery. Rate of R1-R0 was 35% (n = 6/17). Median overall survival was 31 months (95% CI; 4-undefined) for the six patients with R0/R1 resection and 21 months (95% CI; 4-25) for the 11 patients without resection or R2 resection (logrank p = 0.044).
Conclusion: After neoadjuvant chemotherapy, IRE could provide R0 or R1 resection in 35% of LAPC, which seems to be associated with higher OS.
Clinical relevance statement: After induction chemotherapy, stable locally advanced pancreatic cancers can be treated by irreversible electroporation, which could lead to a secondary 35% rate of R0 or R1 surgical resection which may be associated with a significantly higher overall survival.
Key points: • In cases of unresectable LAPC (locally advanced pancreatic cancer), percutaneous irreversible electroporation (pIRE) is feasible (100% success rate of the procedure), but is associated with a 58% rate of grade 3-4 adverse events. • In patients with unresectable LAPC, pIRE could lead 35% of patients to R0-R1 surgical resection. • From IRE, median overall survival was 31 months (95% CI; 4-undefined) for the patients with R0/R1 resection and 21 months (95% CI; 4-25) for the patients without resection or R2 resection (logrank p = 0.044).
期刊介绍:
European Radiology (ER) continuously updates scientific knowledge in radiology by publication of strong original articles and state-of-the-art reviews written by leading radiologists. A well balanced combination of review articles, original papers, short communications from European radiological congresses and information on society matters makes ER an indispensable source for current information in this field.
This is the Journal of the European Society of Radiology, and the official journal of a number of societies.
From 2004-2008 supplements to European Radiology were published under its companion, European Radiology Supplements, ISSN 1613-3749.


 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
