Karl J Jepsen, Erin M R Bigelow, Robert W Goulet, Bonnie T Nolan, Michael A Casden, Kathryn Kennedy, Samantha Hertz, Chandan Kadur, Gregory A Clines, Aleda M Leis, Carrie A Karvonen-Gutierrez, Todd L Bredbenner
{"title":"导致成年白人女性和男性 FN BMD 与全骨强度之间性别特异性关联的结构差异。","authors":"Karl J Jepsen, Erin M R Bigelow, Robert W Goulet, Bonnie T Nolan, Michael A Casden, Kathryn Kennedy, Samantha Hertz, Chandan Kadur, Gregory A Clines, Aleda M Leis, Carrie A Karvonen-Gutierrez, Todd L Bredbenner","doi":"10.1093/jbmrpl/ziae013","DOIUrl":null,"url":null,"abstract":"<p><p>Hip areal BMD (aBMD) is widely used to identify individuals with increased fracture risk. Low aBMD indicates low strength, but this association differs by sex with men showing greater strength for a given aBMD than women. To better understand the structural basis giving rise to this sex-specific discrepancy, cadaveric proximal femurs from White female and male donors were imaged using nano-CT and loaded in a sideways fall configuration to assess strength. FN pseudoDXA images were generated to identify associations among structure, aBMD, and strength that differ by sex. Strength correlated significantly with pseudoDXA aBMD for females (<i>R</i><sup>2</sup> = 0.468, <i>P</i> < .001) and males (<i>R</i><sup>2</sup> = 0.393, <i>P</i> < .001), but the elevations (<i>y</i>-intercepts) of the linear regressions differed between sexes (<i>P</i> < .001). Male proximal femurs were 1045 N stronger than females for a given pseudoDXA aBMD. However, strength correlated with pseudoDXA BMC for females (<i>R</i><sup>2</sup> = 0.433, <i>P</i> < .001) and males (<i>R</i><sup>2</sup> = 0.443, <i>P</i> < .001) but without significant slope (<i>P</i> = .431) or elevation (<i>P</i> = .058) differences. Dividing pseudoDXA BMC by FN-width, total cross-sectional area, or FN-volume led to significantly different associations between strength and the size-adjusted BMC measures for women and men. Three structural differences were identified that differentially affected aBMD and strength for women and men: First, men had more bone mass per unit volume than women; second, different cross-sectional shapes resulted in larger proportions of bone mass orthogonal to the DXA image for men than women; and third, men and women had different proportions of cortical and trabecular bone relative to BMC. Thus, the proximal femurs of women were not smaller versions of men but were constructed in fundamentally different manners. Dividing BMC by a bone size measure was responsible for the sex-specific associations between hip aBMD and strength. Thus, a new approach for adjusting measures of bone mass for bone size and stature is warranted.</p>","PeriodicalId":14611,"journal":{"name":"JBMR Plus","volume":"8 4","pages":"ziae013"},"PeriodicalIF":2.4000,"publicationDate":"2024-01-30","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10958990/pdf/","citationCount":"0","resultStr":"{\"title\":\"Structural differences contributing to sex-specific associations between FN BMD and whole-bone strength for adult White women and men.\",\"authors\":\"Karl J Jepsen, Erin M R Bigelow, Robert W Goulet, Bonnie T Nolan, Michael A Casden, Kathryn Kennedy, Samantha Hertz, Chandan Kadur, Gregory A Clines, Aleda M Leis, Carrie A Karvonen-Gutierrez, Todd L Bredbenner\",\"doi\":\"10.1093/jbmrpl/ziae013\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>Hip areal BMD (aBMD) is widely used to identify individuals with increased fracture risk. Low aBMD indicates low strength, but this association differs by sex with men showing greater strength for a given aBMD than women. To better understand the structural basis giving rise to this sex-specific discrepancy, cadaveric proximal femurs from White female and male donors were imaged using nano-CT and loaded in a sideways fall configuration to assess strength. FN pseudoDXA images were generated to identify associations among structure, aBMD, and strength that differ by sex. Strength correlated significantly with pseudoDXA aBMD for females (<i>R</i><sup>2</sup> = 0.468, <i>P</i> < .001) and males (<i>R</i><sup>2</sup> = 0.393, <i>P</i> < .001), but the elevations (<i>y</i>-intercepts) of the linear regressions differed between sexes (<i>P</i> < .001). Male proximal femurs were 1045 N stronger than females for a given pseudoDXA aBMD. However, strength correlated with pseudoDXA BMC for females (<i>R</i><sup>2</sup> = 0.433, <i>P</i> < .001) and males (<i>R</i><sup>2</sup> = 0.443, <i>P</i> < .001) but without significant slope (<i>P</i> = .431) or elevation (<i>P</i> = .058) differences. Dividing pseudoDXA BMC by FN-width, total cross-sectional area, or FN-volume led to significantly different associations between strength and the size-adjusted BMC measures for women and men. Three structural differences were identified that differentially affected aBMD and strength for women and men: First, men had more bone mass per unit volume than women; second, different cross-sectional shapes resulted in larger proportions of bone mass orthogonal to the DXA image for men than women; and third, men and women had different proportions of cortical and trabecular bone relative to BMC. Thus, the proximal femurs of women were not smaller versions of men but were constructed in fundamentally different manners. Dividing BMC by a bone size measure was responsible for the sex-specific associations between hip aBMD and strength. Thus, a new approach for adjusting measures of bone mass for bone size and stature is warranted.</p>\",\"PeriodicalId\":14611,\"journal\":{\"name\":\"JBMR Plus\",\"volume\":\"8 4\",\"pages\":\"ziae013\"},\"PeriodicalIF\":2.4000,\"publicationDate\":\"2024-01-30\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10958990/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"JBMR Plus\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1093/jbmrpl/ziae013\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2024/4/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q2\",\"JCRName\":\"ENDOCRINOLOGY & METABOLISM\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"JBMR Plus","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1093/jbmrpl/ziae013","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/4/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"ENDOCRINOLOGY & METABOLISM","Score":null,"Total":0}
Structural differences contributing to sex-specific associations between FN BMD and whole-bone strength for adult White women and men.
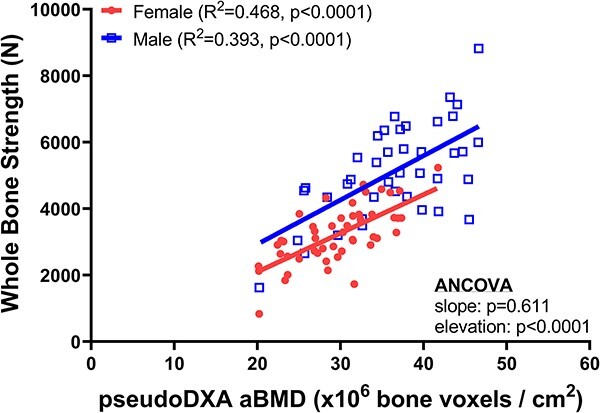
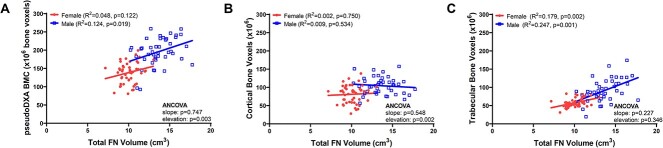
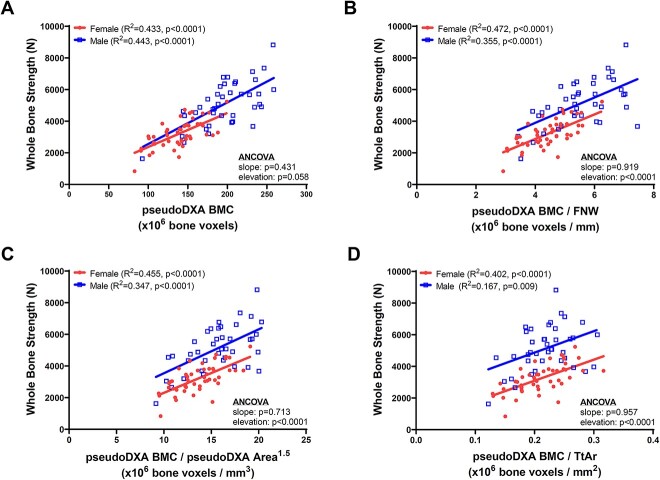
Hip areal BMD (aBMD) is widely used to identify individuals with increased fracture risk. Low aBMD indicates low strength, but this association differs by sex with men showing greater strength for a given aBMD than women. To better understand the structural basis giving rise to this sex-specific discrepancy, cadaveric proximal femurs from White female and male donors were imaged using nano-CT and loaded in a sideways fall configuration to assess strength. FN pseudoDXA images were generated to identify associations among structure, aBMD, and strength that differ by sex. Strength correlated significantly with pseudoDXA aBMD for females (R2 = 0.468, P < .001) and males (R2 = 0.393, P < .001), but the elevations (y-intercepts) of the linear regressions differed between sexes (P < .001). Male proximal femurs were 1045 N stronger than females for a given pseudoDXA aBMD. However, strength correlated with pseudoDXA BMC for females (R2 = 0.433, P < .001) and males (R2 = 0.443, P < .001) but without significant slope (P = .431) or elevation (P = .058) differences. Dividing pseudoDXA BMC by FN-width, total cross-sectional area, or FN-volume led to significantly different associations between strength and the size-adjusted BMC measures for women and men. Three structural differences were identified that differentially affected aBMD and strength for women and men: First, men had more bone mass per unit volume than women; second, different cross-sectional shapes resulted in larger proportions of bone mass orthogonal to the DXA image for men than women; and third, men and women had different proportions of cortical and trabecular bone relative to BMC. Thus, the proximal femurs of women were not smaller versions of men but were constructed in fundamentally different manners. Dividing BMC by a bone size measure was responsible for the sex-specific associations between hip aBMD and strength. Thus, a new approach for adjusting measures of bone mass for bone size and stature is warranted.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
