Lucas Simões Arrebola PhD , Toby O. Smith PhD , Vanessa Gonçalves Coutinho de Oliveira MSc , Pedro Rizzi de Oliveira MSc , Paloma Yan Lam Wun , Rogério Teixeira de Carvalho PhD , Carlos Eduardo Pinfildi PhD
{"title":"对髌骨外侧脱位患者进行髋关节和膝关节联合强化治疗与膝关节强化治疗的比较:单盲、优越性随机对照试验","authors":"Lucas Simões Arrebola PhD , Toby O. Smith PhD , Vanessa Gonçalves Coutinho de Oliveira MSc , Pedro Rizzi de Oliveira MSc , Paloma Yan Lam Wun , Rogério Teixeira de Carvalho PhD , Carlos Eduardo Pinfildi PhD","doi":"10.1016/j.arrct.2024.100334","DOIUrl":null,"url":null,"abstract":"<div><h3>Objective</h3><p>To investigate whether a combined hip and knee muscle strengthening program is superior to a knee strengthening program for people after lateral patellar dislocation (LPD).</p></div><div><h3>Design</h3><p>Single-blind, superiority, randomized controlled trial with 48 weeks follow-up.</p></div><div><h3>Setting</h3><p>Physiotherapy out-patient clinic.</p></div><div><h3>Participants</h3><p>Forty individuals aged 16 or older, with a history of non-traumatic LPD were randomized to a knee-based strengthening (KBSG) or quadriceps and hip strengthening exercise (HQSG) program (N=40). Inclusion criteria included a positive apprehension sign, pain on palpation along the medial retinaculum, and J sign. Exclusion criteria included restricted range of motion (<90° knee flexion), and traumatic or postsurgical LPD.</p></div><div><h3>Interventions</h3><p>Concealed randomization was performed using random permuted blocks of size 4. Individuals received their corresponding exercise program according to randomization and group allocation: knee-based strengthening (n=20) or combined hip and quadriceps strengthening (n=20) twice weekly for 8 weeks over 16 appointments.</p></div><div><h3>Main Outcome Measures</h3><p>Primary outcome was the Lysholm Knee Score. Secondary outcomes included Numerical Pain Ratings Scale (NPRS) at rest and during effort, Norwich Patellar Instability Score (NPIS), Kujala Anterior Knee Pain Scale (AKPS), Lower Extremity Functional Scale (LEFS), 4 domains of the WHOQOL-Bref, and recurrence rate. Patient-reported outcome measures were assessed from the baseline to 48 weeks. Assessments were performed by a physiotherapist who was blinded to the group allocation. Data were analyzed by using a repeated-measures ANOVA model with Tukey's post hoc test after an intention-to-treat principle.</p></div><div><h3>Results</h3><p>At the primary time-point of 8 weeks, there were no substantial between-group differences in the Lysholm Knee Score: mean difference=-6.8 (95% CI -14.3 to 3.7); NPIS: mean difference=23.5 (95% CI 5.6 to 41.3); AKPS: mean difference=-1.54 (95% CI -8.6 to 5.6), NPRS at rest and during effort (mean difference=0.32 (95% CI -0.37 to 1); and mean difference=0.68 (95% CI -0.9 to 1.86); LEFS mean difference=-1.08 (95% CI -5.9 to 2.4), WHOQOL-Bref domains (physical health: mean difference=-0.12, (95% CI -1.26 to 1.02); psychological: mean difference=-0.32 (95% CI -2.04 to 1.4); social relations: mean difference=-0.7 (95% CI -2.2 to 0.82); environment: mean difference=0.44 (95% CI -1 to 1.9), and recurrence rate (<em>P</em>=.69).</p></div><div><h3>Conclusion</h3><p>This study indicates that combined hip and knee muscle strengthening is not superior to knee-based strengthening for LPD treatment. The limitations stemming from the underpowered nature of the trial must be acknowledged, concerning the potential oversight of moderate intervention effects.</p></div>","PeriodicalId":72291,"journal":{"name":"Archives of rehabilitation research and clinical translation","volume":"6 2","pages":"Article 100334"},"PeriodicalIF":1.9000,"publicationDate":"2024-06-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.sciencedirect.com/science/article/pii/S2590109524000247/pdfft?md5=3f3c71208d1d61d4107561ecb68ca5f4&pid=1-s2.0-S2590109524000247-main.pdf","citationCount":"0","resultStr":"{\"title\":\"Combined Hip and Knee Strengthening Compared With Knee Strengthening for Individuals With Lateral Patellar Dislocation: A Single-blind, Superiority, Randomized Controlled Trial\",\"authors\":\"Lucas Simões Arrebola PhD , Toby O. Smith PhD , Vanessa Gonçalves Coutinho de Oliveira MSc , Pedro Rizzi de Oliveira MSc , Paloma Yan Lam Wun , Rogério Teixeira de Carvalho PhD , Carlos Eduardo Pinfildi PhD\",\"doi\":\"10.1016/j.arrct.2024.100334\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<div><h3>Objective</h3><p>To investigate whether a combined hip and knee muscle strengthening program is superior to a knee strengthening program for people after lateral patellar dislocation (LPD).</p></div><div><h3>Design</h3><p>Single-blind, superiority, randomized controlled trial with 48 weeks follow-up.</p></div><div><h3>Setting</h3><p>Physiotherapy out-patient clinic.</p></div><div><h3>Participants</h3><p>Forty individuals aged 16 or older, with a history of non-traumatic LPD were randomized to a knee-based strengthening (KBSG) or quadriceps and hip strengthening exercise (HQSG) program (N=40). Inclusion criteria included a positive apprehension sign, pain on palpation along the medial retinaculum, and J sign. Exclusion criteria included restricted range of motion (<90° knee flexion), and traumatic or postsurgical LPD.</p></div><div><h3>Interventions</h3><p>Concealed randomization was performed using random permuted blocks of size 4. Individuals received their corresponding exercise program according to randomization and group allocation: knee-based strengthening (n=20) or combined hip and quadriceps strengthening (n=20) twice weekly for 8 weeks over 16 appointments.</p></div><div><h3>Main Outcome Measures</h3><p>Primary outcome was the Lysholm Knee Score. Secondary outcomes included Numerical Pain Ratings Scale (NPRS) at rest and during effort, Norwich Patellar Instability Score (NPIS), Kujala Anterior Knee Pain Scale (AKPS), Lower Extremity Functional Scale (LEFS), 4 domains of the WHOQOL-Bref, and recurrence rate. Patient-reported outcome measures were assessed from the baseline to 48 weeks. Assessments were performed by a physiotherapist who was blinded to the group allocation. Data were analyzed by using a repeated-measures ANOVA model with Tukey's post hoc test after an intention-to-treat principle.</p></div><div><h3>Results</h3><p>At the primary time-point of 8 weeks, there were no substantial between-group differences in the Lysholm Knee Score: mean difference=-6.8 (95% CI -14.3 to 3.7); NPIS: mean difference=23.5 (95% CI 5.6 to 41.3); AKPS: mean difference=-1.54 (95% CI -8.6 to 5.6), NPRS at rest and during effort (mean difference=0.32 (95% CI -0.37 to 1); and mean difference=0.68 (95% CI -0.9 to 1.86); LEFS mean difference=-1.08 (95% CI -5.9 to 2.4), WHOQOL-Bref domains (physical health: mean difference=-0.12, (95% CI -1.26 to 1.02); psychological: mean difference=-0.32 (95% CI -2.04 to 1.4); social relations: mean difference=-0.7 (95% CI -2.2 to 0.82); environment: mean difference=0.44 (95% CI -1 to 1.9), and recurrence rate (<em>P</em>=.69).</p></div><div><h3>Conclusion</h3><p>This study indicates that combined hip and knee muscle strengthening is not superior to knee-based strengthening for LPD treatment. The limitations stemming from the underpowered nature of the trial must be acknowledged, concerning the potential oversight of moderate intervention effects.</p></div>\",\"PeriodicalId\":72291,\"journal\":{\"name\":\"Archives of rehabilitation research and clinical translation\",\"volume\":\"6 2\",\"pages\":\"Article 100334\"},\"PeriodicalIF\":1.9000,\"publicationDate\":\"2024-06-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.sciencedirect.com/science/article/pii/S2590109524000247/pdfft?md5=3f3c71208d1d61d4107561ecb68ca5f4&pid=1-s2.0-S2590109524000247-main.pdf\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Archives of rehabilitation research and clinical translation\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://www.sciencedirect.com/science/article/pii/S2590109524000247\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q2\",\"JCRName\":\"REHABILITATION\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Archives of rehabilitation research and clinical translation","FirstCategoryId":"1085","ListUrlMain":"https://www.sciencedirect.com/science/article/pii/S2590109524000247","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"REHABILITATION","Score":null,"Total":0}
引用次数: 0
摘要
研究对象40名年龄在16岁或16岁以上、有非创伤性髌骨脱位病史的患者,随机接受膝关节强化训练(KBSG)或股四头肌和髋关节强化训练(HQSG)(N=40)。纳入标准包括忧虑征阳性、沿内侧腱网触诊疼痛和 J 征。排除标准包括活动范围受限(膝关节屈曲 90°)、外伤性或手术后 LPD。个人根据随机化和组别分配接受相应的锻炼计划:膝关节强化训练(20 人)或髋关节和股四头肌联合强化训练(20 人),每周两次,每次 8 周,共 16 次预约。次要结果包括休息和用力时的数字疼痛评分量表(NPRS)、诺维奇髌骨不稳定性评分(NPIS)、库亚拉膝关节前部疼痛量表(AKPS)、下肢功能量表(LEFS)、WHOQOL-Bref 的 4 个领域以及复发率。患者报告结果的评估时间为基线至 48 周。评估由一名物理治疗师进行,该物理治疗师对组别分配设置了盲法。结果在8周的主要时间点,Lysholm膝关节评分在组间没有实质性差异:平均差异=-6.8 (95% CI -14.3 to 3.7);NPIS:平均差异=23.5 (95% CI 5.6 to 41.3);AKPS:平均差异=-1.54 (95% CI -8.6 to 5.6);休息时和用力时的 NPRS(平均差异=0.32 (95% CI -0.37 to 1);平均差异=0.68 (95% CI -0. 9 to 1.86);Lysholm 膝关节评分:平均差异=-6.9至1.86);LEFS平均差=-1.08(95% CI-5.9至2.4),WHOQOL-Bref域(身体健康:平均差=-0.12,(95% CI-1.26至1.02);心理:平均差=-0.32(95% CI-2.04至1.4);社会关系:平均差=-0.7 (95% CI -2.2 to 0.82);环境:平均差异=0.44 (95% CI -1 to 1.9),以及复发率(P=.69)。必须承认的是,由于试验的动力不足,可能会忽略中等程度的干预效果。
Combined Hip and Knee Strengthening Compared With Knee Strengthening for Individuals With Lateral Patellar Dislocation: A Single-blind, Superiority, Randomized Controlled Trial
Objective
To investigate whether a combined hip and knee muscle strengthening program is superior to a knee strengthening program for people after lateral patellar dislocation (LPD).
Design
Single-blind, superiority, randomized controlled trial with 48 weeks follow-up.
Setting
Physiotherapy out-patient clinic.
Participants
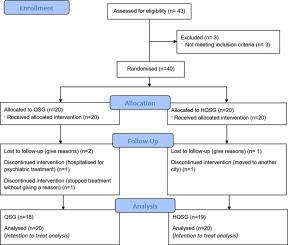
Forty individuals aged 16 or older, with a history of non-traumatic LPD were randomized to a knee-based strengthening (KBSG) or quadriceps and hip strengthening exercise (HQSG) program (N=40). Inclusion criteria included a positive apprehension sign, pain on palpation along the medial retinaculum, and J sign. Exclusion criteria included restricted range of motion (<90° knee flexion), and traumatic or postsurgical LPD.
Interventions
Concealed randomization was performed using random permuted blocks of size 4. Individuals received their corresponding exercise program according to randomization and group allocation: knee-based strengthening (n=20) or combined hip and quadriceps strengthening (n=20) twice weekly for 8 weeks over 16 appointments.
Main Outcome Measures
Primary outcome was the Lysholm Knee Score. Secondary outcomes included Numerical Pain Ratings Scale (NPRS) at rest and during effort, Norwich Patellar Instability Score (NPIS), Kujala Anterior Knee Pain Scale (AKPS), Lower Extremity Functional Scale (LEFS), 4 domains of the WHOQOL-Bref, and recurrence rate. Patient-reported outcome measures were assessed from the baseline to 48 weeks. Assessments were performed by a physiotherapist who was blinded to the group allocation. Data were analyzed by using a repeated-measures ANOVA model with Tukey's post hoc test after an intention-to-treat principle.
Results
At the primary time-point of 8 weeks, there were no substantial between-group differences in the Lysholm Knee Score: mean difference=-6.8 (95% CI -14.3 to 3.7); NPIS: mean difference=23.5 (95% CI 5.6 to 41.3); AKPS: mean difference=-1.54 (95% CI -8.6 to 5.6), NPRS at rest and during effort (mean difference=0.32 (95% CI -0.37 to 1); and mean difference=0.68 (95% CI -0.9 to 1.86); LEFS mean difference=-1.08 (95% CI -5.9 to 2.4), WHOQOL-Bref domains (physical health: mean difference=-0.12, (95% CI -1.26 to 1.02); psychological: mean difference=-0.32 (95% CI -2.04 to 1.4); social relations: mean difference=-0.7 (95% CI -2.2 to 0.82); environment: mean difference=0.44 (95% CI -1 to 1.9), and recurrence rate (P=.69).
Conclusion
This study indicates that combined hip and knee muscle strengthening is not superior to knee-based strengthening for LPD treatment. The limitations stemming from the underpowered nature of the trial must be acknowledged, concerning the potential oversight of moderate intervention effects.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
