Long Vu, Siran M Koroukian, Sara L Douglas, Hannah L Fein, David F Warner, Nicholas K Schiltz, Jennifer Cullen, Cynthia Owusu, Martha Sajatovic, Johnie Rose, Richard Martin
{"title":"利用美国养老院癌症患者的管理数据了解少于六个月预后的效用。","authors":"Long Vu, Siran M Koroukian, Sara L Douglas, Hannah L Fein, David F Warner, Nicholas K Schiltz, Jennifer Cullen, Cynthia Owusu, Martha Sajatovic, Johnie Rose, Richard Martin","doi":"10.1089/pmr.2023.0047","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>There is a dearth of studies evaluating the utility of reporting prognostication among nursing home (NH) residents with cancer.</p><p><strong>Objective: </strong>To study factors associated with documented less than six-month prognosis, and its relationship with end-of-life (EOL) care quality measures among residents with cancer.</p><p><strong>Methods: </strong>The Surveillance, Epidemiology, and End Results linked with Medicare, and the Minimum Data Set databases was used to identify 20,397 NH residents in the United States with breast, colorectal, lung, pancreatic, or prostate cancer who died between July 2016 and December 2018. Of these, 2205 residents (10.8%) were documented with less than six-month prognosis upon NH admission. Main outcomes were more than one hospitalization, more than one emergency department visit, and any intensive care unit admission within the last 30 days of life as aggressive EOL care markers, as well as admission to hospice, receipt of advance care planning and palliative care, and survival. Specificity and sensitivity of prognosis were assessed using six-month mortality as the outcome. Propensity score matching adjusted for selection biases, and logistic regression examined association.</p><p><strong>Results: </strong>Specificity and sensitivity of documented less than six-month prognosis for mortality were 94.2% and 13.7%, respectively. Residents with documented less than six-month prognosis had greater odds of being admitted to hospice than those without (adjusted odds ratio: 3.27, 95% confidence interval: 2.86-3.62), and lower odds to receive aggressive EOL care.</p><p><strong>Conclusion: </strong>In this cohort study, documented less than six-month prognosis was associated with less aggressive EOL care. Despite its high specificity, however, low sensitivity limits its utility to operationalize care on a larger population of residents with terminal illness.</p>","PeriodicalId":74394,"journal":{"name":"Palliative medicine reports","volume":"5 1","pages":"127-135"},"PeriodicalIF":1.3000,"publicationDate":"2024-03-28","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10979665/pdf/","citationCount":"0","resultStr":"{\"title\":\"Understanding the Utility of Less Than Six-Month Prognosis Using Administrative Data Among U.S. Nursing Home Residents With Cancer.\",\"authors\":\"Long Vu, Siran M Koroukian, Sara L Douglas, Hannah L Fein, David F Warner, Nicholas K Schiltz, Jennifer Cullen, Cynthia Owusu, Martha Sajatovic, Johnie Rose, Richard Martin\",\"doi\":\"10.1089/pmr.2023.0047\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>There is a dearth of studies evaluating the utility of reporting prognostication among nursing home (NH) residents with cancer.</p><p><strong>Objective: </strong>To study factors associated with documented less than six-month prognosis, and its relationship with end-of-life (EOL) care quality measures among residents with cancer.</p><p><strong>Methods: </strong>The Surveillance, Epidemiology, and End Results linked with Medicare, and the Minimum Data Set databases was used to identify 20,397 NH residents in the United States with breast, colorectal, lung, pancreatic, or prostate cancer who died between July 2016 and December 2018. Of these, 2205 residents (10.8%) were documented with less than six-month prognosis upon NH admission. Main outcomes were more than one hospitalization, more than one emergency department visit, and any intensive care unit admission within the last 30 days of life as aggressive EOL care markers, as well as admission to hospice, receipt of advance care planning and palliative care, and survival. Specificity and sensitivity of prognosis were assessed using six-month mortality as the outcome. Propensity score matching adjusted for selection biases, and logistic regression examined association.</p><p><strong>Results: </strong>Specificity and sensitivity of documented less than six-month prognosis for mortality were 94.2% and 13.7%, respectively. Residents with documented less than six-month prognosis had greater odds of being admitted to hospice than those without (adjusted odds ratio: 3.27, 95% confidence interval: 2.86-3.62), and lower odds to receive aggressive EOL care.</p><p><strong>Conclusion: </strong>In this cohort study, documented less than six-month prognosis was associated with less aggressive EOL care. Despite its high specificity, however, low sensitivity limits its utility to operationalize care on a larger population of residents with terminal illness.</p>\",\"PeriodicalId\":74394,\"journal\":{\"name\":\"Palliative medicine reports\",\"volume\":\"5 1\",\"pages\":\"127-135\"},\"PeriodicalIF\":1.3000,\"publicationDate\":\"2024-03-28\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10979665/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Palliative medicine reports\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1089/pmr.2023.0047\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2024/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q4\",\"JCRName\":\"HEALTH CARE SCIENCES & SERVICES\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Palliative medicine reports","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1089/pmr.2023.0047","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/1/1 0:00:00","PubModel":"eCollection","JCR":"Q4","JCRName":"HEALTH CARE SCIENCES & SERVICES","Score":null,"Total":0}
Understanding the Utility of Less Than Six-Month Prognosis Using Administrative Data Among U.S. Nursing Home Residents With Cancer.
Background: There is a dearth of studies evaluating the utility of reporting prognostication among nursing home (NH) residents with cancer.
Objective: To study factors associated with documented less than six-month prognosis, and its relationship with end-of-life (EOL) care quality measures among residents with cancer.
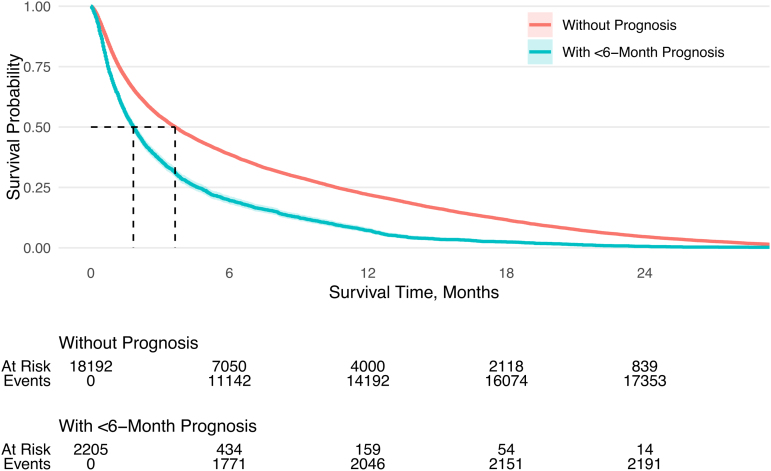
Methods: The Surveillance, Epidemiology, and End Results linked with Medicare, and the Minimum Data Set databases was used to identify 20,397 NH residents in the United States with breast, colorectal, lung, pancreatic, or prostate cancer who died between July 2016 and December 2018. Of these, 2205 residents (10.8%) were documented with less than six-month prognosis upon NH admission. Main outcomes were more than one hospitalization, more than one emergency department visit, and any intensive care unit admission within the last 30 days of life as aggressive EOL care markers, as well as admission to hospice, receipt of advance care planning and palliative care, and survival. Specificity and sensitivity of prognosis were assessed using six-month mortality as the outcome. Propensity score matching adjusted for selection biases, and logistic regression examined association.
Results: Specificity and sensitivity of documented less than six-month prognosis for mortality were 94.2% and 13.7%, respectively. Residents with documented less than six-month prognosis had greater odds of being admitted to hospice than those without (adjusted odds ratio: 3.27, 95% confidence interval: 2.86-3.62), and lower odds to receive aggressive EOL care.
Conclusion: In this cohort study, documented less than six-month prognosis was associated with less aggressive EOL care. Despite its high specificity, however, low sensitivity limits its utility to operationalize care on a larger population of residents with terminal illness.



 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
