Yu Chen , Lung-Yi Mak , Mary H.Y. Tang , Jingyi Yang , Chun Bong Chow , Ai-Ming Tan , Tao Lyu , Juan Wu , Qingjuan Huang , Hai-Bo Huang , Ka-Shing Cheung , Man-Fung Yuen , Wai-Kay Seto
{"title":"产后立即停用替诺福韦酯不会增加高病毒血症慢性乙型肝炎孕产妇的病毒学或临床复发风险","authors":"Yu Chen , Lung-Yi Mak , Mary H.Y. Tang , Jingyi Yang , Chun Bong Chow , Ai-Ming Tan , Tao Lyu , Juan Wu , Qingjuan Huang , Hai-Bo Huang , Ka-Shing Cheung , Man-Fung Yuen , Wai-Kay Seto","doi":"10.1016/j.jhepr.2024.101050","DOIUrl":null,"url":null,"abstract":"<div><h3>Background & Aims</h3><p>Peripartum prophylaxis (PP) with tenofovir disoproxil fumarate (TDF) is the standard of care to prevent mother-to-child transmission of chronic hepatitis B (CHB) infection in mothers who are highly viremic. We investigated the maternal and infant outcomes in a large Chinese cohort of TDF-treated CHB pregnant participants.</p></div><div><h3>Methods</h3><p>In this prospective study, treatment-naive mothers with CHB and highly viremic (HBV DNA ≥200,000 IU/ml) but without cirrhosis were treated with TDF at 24–28 weeks of pregnancy. In accordance with Chinese CHB guidelines, TDF was stopped at delivery or ≥4 weeks postpartum. Serum HBV DNA and alanine aminotransferase were monitored every 6–8 weeks to determine virological relapse (VR). Infants received standard neonatal immunization, and HBV serology was checked at 7–12 months of age.</p></div><div><h3>Results</h3><p>Among 330 participants recruited (median age 30, 82.7% HBeAg+, median HBV DNA 7.82 log IU/ml), TDF was stopped at delivery in 66.4% and at ≥4 weeks in 33.6%. VR was observed in 98.3%, among which 11.6% were retreated with TDF. Timing of TDF cessation did not alter the risk of VR (99.0 <em>vs</em>. 96.9%), clinical relapse (19.5 <em>vs</em>. 14.3%), or retreatment (12.6 <em>vs</em>. 10.1%) (all <em>p</em> > 0.05). A similar proportion of patients developed alanine aminotransferase flare five times (1.1 <em>vs</em>. 2.1%; <em>p</em> = 0.464) and 10 times (0.5 <em>vs</em>. 0%; <em>p</em> = 0.669) above the upper limit of normal (ULN) in the early withdrawal and late withdrawal groups, respectively. No infants developed HBsAg-positivity.</p></div><div><h3>Conclusions</h3><p>PP-TDF and neonatal immunization were highly effective in preventing mother-to-child transmission of HBV in mothers who are highly viremic. Timing of cessation of PP-TDF did not affect the risk of VR or retreatment.</p></div><div><h3>Impact and Implications</h3><p>In pregnant mothers with chronic hepatitis B infection who are started on peripartum tenofovir to prevent mother-to-child-transmission (MTCT), the optimal timing for antiviral withdrawal during the postpartum period remains unknown. This prospective study demonstrates that stopping tenofovir immediately at delivery, compared with longer treatment duration of tenofovir, did not lead to an increased risk of virological relapse, retreatment, or transmission of the virus to the baby. Shortening the duration of peripartum antiviral prophylaxis from 12 weeks to immediately after delivery can be considered. The immediate withdrawal of peripartum tenofovir, combined with standard neonatal immunization schemes, is 100% effective in preventing MTCT among pregnant mothers with CHB who are highly viremic, with a high rate of vaccine response in infants.</p></div>","PeriodicalId":14764,"journal":{"name":"JHEP Reports","volume":"6 5","pages":"Article 101050"},"PeriodicalIF":7.5000,"publicationDate":"2024-05-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.sciencedirect.com/science/article/pii/S258955592400051X/pdfft?md5=7c823a326115936fcf170ca16dbfa557&pid=1-s2.0-S258955592400051X-main.pdf","citationCount":"0","resultStr":"{\"title\":\"Immediate postpartum cessation of tenofovir did not increase risk of virological or clinical relapse in highly viremic pregnant mothers with chronic hepatitis B infection\",\"authors\":\"Yu Chen , Lung-Yi Mak , Mary H.Y. Tang , Jingyi Yang , Chun Bong Chow , Ai-Ming Tan , Tao Lyu , Juan Wu , Qingjuan Huang , Hai-Bo Huang , Ka-Shing Cheung , Man-Fung Yuen , Wai-Kay Seto\",\"doi\":\"10.1016/j.jhepr.2024.101050\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<div><h3>Background & Aims</h3><p>Peripartum prophylaxis (PP) with tenofovir disoproxil fumarate (TDF) is the standard of care to prevent mother-to-child transmission of chronic hepatitis B (CHB) infection in mothers who are highly viremic. We investigated the maternal and infant outcomes in a large Chinese cohort of TDF-treated CHB pregnant participants.</p></div><div><h3>Methods</h3><p>In this prospective study, treatment-naive mothers with CHB and highly viremic (HBV DNA ≥200,000 IU/ml) but without cirrhosis were treated with TDF at 24–28 weeks of pregnancy. In accordance with Chinese CHB guidelines, TDF was stopped at delivery or ≥4 weeks postpartum. Serum HBV DNA and alanine aminotransferase were monitored every 6–8 weeks to determine virological relapse (VR). Infants received standard neonatal immunization, and HBV serology was checked at 7–12 months of age.</p></div><div><h3>Results</h3><p>Among 330 participants recruited (median age 30, 82.7% HBeAg+, median HBV DNA 7.82 log IU/ml), TDF was stopped at delivery in 66.4% and at ≥4 weeks in 33.6%. VR was observed in 98.3%, among which 11.6% were retreated with TDF. Timing of TDF cessation did not alter the risk of VR (99.0 <em>vs</em>. 96.9%), clinical relapse (19.5 <em>vs</em>. 14.3%), or retreatment (12.6 <em>vs</em>. 10.1%) (all <em>p</em> > 0.05). A similar proportion of patients developed alanine aminotransferase flare five times (1.1 <em>vs</em>. 2.1%; <em>p</em> = 0.464) and 10 times (0.5 <em>vs</em>. 0%; <em>p</em> = 0.669) above the upper limit of normal (ULN) in the early withdrawal and late withdrawal groups, respectively. No infants developed HBsAg-positivity.</p></div><div><h3>Conclusions</h3><p>PP-TDF and neonatal immunization were highly effective in preventing mother-to-child transmission of HBV in mothers who are highly viremic. Timing of cessation of PP-TDF did not affect the risk of VR or retreatment.</p></div><div><h3>Impact and Implications</h3><p>In pregnant mothers with chronic hepatitis B infection who are started on peripartum tenofovir to prevent mother-to-child-transmission (MTCT), the optimal timing for antiviral withdrawal during the postpartum period remains unknown. This prospective study demonstrates that stopping tenofovir immediately at delivery, compared with longer treatment duration of tenofovir, did not lead to an increased risk of virological relapse, retreatment, or transmission of the virus to the baby. Shortening the duration of peripartum antiviral prophylaxis from 12 weeks to immediately after delivery can be considered. The immediate withdrawal of peripartum tenofovir, combined with standard neonatal immunization schemes, is 100% effective in preventing MTCT among pregnant mothers with CHB who are highly viremic, with a high rate of vaccine response in infants.</p></div>\",\"PeriodicalId\":14764,\"journal\":{\"name\":\"JHEP Reports\",\"volume\":\"6 5\",\"pages\":\"Article 101050\"},\"PeriodicalIF\":7.5000,\"publicationDate\":\"2024-05-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.sciencedirect.com/science/article/pii/S258955592400051X/pdfft?md5=7c823a326115936fcf170ca16dbfa557&pid=1-s2.0-S258955592400051X-main.pdf\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"JHEP Reports\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://www.sciencedirect.com/science/article/pii/S258955592400051X\",\"RegionNum\":1,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2024/2/28 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q1\",\"JCRName\":\"GASTROENTEROLOGY & HEPATOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"JHEP Reports","FirstCategoryId":"3","ListUrlMain":"https://www.sciencedirect.com/science/article/pii/S258955592400051X","RegionNum":1,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/2/28 0:00:00","PubModel":"Epub","JCR":"Q1","JCRName":"GASTROENTEROLOGY & HEPATOLOGY","Score":null,"Total":0}
引用次数: 0
摘要
背景& 目的富马酸替诺福韦二吡呋酯(TDF)产前预防(PP)是预防高病毒血症母亲感染慢性乙型肝炎(CHB)后母婴传播的标准治疗方法。在这项前瞻性研究中,未经治疗的慢性乙型肝炎高病毒血症(HBV DNA ≥200,000 IU/ml)但无肝硬化的母亲在怀孕 24-28 周时接受了 TDF 治疗。根据中国慢性阻塞性肺病指南,TDF在分娩时或产后≥4周时停用。每6-8周监测一次血清HBV DNA和丙氨酸氨基转移酶,以确定病毒学复发(VR)。结果在招募的 330 名参与者中(中位年龄 30 岁,82.7% HBeAg+,中位 HBV DNA 7.82 log IU/ml),66.4% 在分娩时停用了 TDF,33.6% 在≥4 周时停用了 TDF。98.3%的患者出现了 VR,其中 11.6%的患者再次接受了 TDF 治疗。停用 TDF 的时间并不会改变 VR(99.0% vs. 96.9%)、临床复发(19.5% vs. 14.3%)或再治疗(12.6% vs. 10.1%)的风险(所有 p > 0.05)。在早期停药组和晚期停药组中,分别有相似比例的患者丙氨酸氨基转移酶超过正常值上限(ULN)5 倍(1.1% 对 2.1%;P = 0.464)和 10 倍(0.5% 对 0%;P = 0.669)。结论 PP-TDF和新生儿免疫接种对预防高病毒血症母亲的HBV母婴传播非常有效。停用 PP-TDF 的时机并不影响 VR 或再治疗的风险。影响和意义在为预防母婴传播(MTCT)而开始使用围产期替诺福韦酯的慢性乙型肝炎感染孕产妇中,产后停用抗病毒药物的最佳时机仍然未知。这项前瞻性研究表明,与延长替诺福韦的治疗时间相比,分娩时立即停用替诺福韦不会导致病毒复发、再治疗或将病毒传播给婴儿的风险增加。可以考虑将围产期抗病毒预防治疗的持续时间从 12 周缩短至分娩后立即停药。立即停用围产期替诺福韦,并结合标准的新生儿免疫计划,对预防高病毒血症合并慢性乙型肝炎孕产妇的母婴传播有效率达 100%,婴儿的疫苗应答率也很高。
Immediate postpartum cessation of tenofovir did not increase risk of virological or clinical relapse in highly viremic pregnant mothers with chronic hepatitis B infection
Background & Aims
Peripartum prophylaxis (PP) with tenofovir disoproxil fumarate (TDF) is the standard of care to prevent mother-to-child transmission of chronic hepatitis B (CHB) infection in mothers who are highly viremic. We investigated the maternal and infant outcomes in a large Chinese cohort of TDF-treated CHB pregnant participants.
Methods
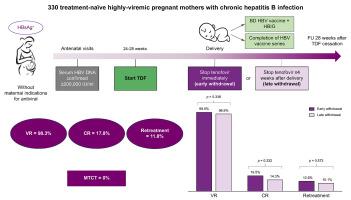
In this prospective study, treatment-naive mothers with CHB and highly viremic (HBV DNA ≥200,000 IU/ml) but without cirrhosis were treated with TDF at 24–28 weeks of pregnancy. In accordance with Chinese CHB guidelines, TDF was stopped at delivery or ≥4 weeks postpartum. Serum HBV DNA and alanine aminotransferase were monitored every 6–8 weeks to determine virological relapse (VR). Infants received standard neonatal immunization, and HBV serology was checked at 7–12 months of age.
Results
Among 330 participants recruited (median age 30, 82.7% HBeAg+, median HBV DNA 7.82 log IU/ml), TDF was stopped at delivery in 66.4% and at ≥4 weeks in 33.6%. VR was observed in 98.3%, among which 11.6% were retreated with TDF. Timing of TDF cessation did not alter the risk of VR (99.0 vs. 96.9%), clinical relapse (19.5 vs. 14.3%), or retreatment (12.6 vs. 10.1%) (all p > 0.05). A similar proportion of patients developed alanine aminotransferase flare five times (1.1 vs. 2.1%; p = 0.464) and 10 times (0.5 vs. 0%; p = 0.669) above the upper limit of normal (ULN) in the early withdrawal and late withdrawal groups, respectively. No infants developed HBsAg-positivity.
Conclusions
PP-TDF and neonatal immunization were highly effective in preventing mother-to-child transmission of HBV in mothers who are highly viremic. Timing of cessation of PP-TDF did not affect the risk of VR or retreatment.
Impact and Implications
In pregnant mothers with chronic hepatitis B infection who are started on peripartum tenofovir to prevent mother-to-child-transmission (MTCT), the optimal timing for antiviral withdrawal during the postpartum period remains unknown. This prospective study demonstrates that stopping tenofovir immediately at delivery, compared with longer treatment duration of tenofovir, did not lead to an increased risk of virological relapse, retreatment, or transmission of the virus to the baby. Shortening the duration of peripartum antiviral prophylaxis from 12 weeks to immediately after delivery can be considered. The immediate withdrawal of peripartum tenofovir, combined with standard neonatal immunization schemes, is 100% effective in preventing MTCT among pregnant mothers with CHB who are highly viremic, with a high rate of vaccine response in infants.
期刊介绍:
JHEP Reports is an open access journal that is affiliated with the European Association for the Study of the Liver (EASL). It serves as a companion journal to the highly respected Journal of Hepatology.
The primary objective of JHEP Reports is to publish original papers and reviews that contribute to the advancement of knowledge in the field of liver diseases. The journal covers a wide range of topics, including basic, translational, and clinical research. It also focuses on global issues in hepatology, with particular emphasis on areas such as clinical trials, novel diagnostics, precision medicine and therapeutics, cancer research, cellular and molecular studies, artificial intelligence, microbiome research, epidemiology, and cutting-edge technologies.
In summary, JHEP Reports is dedicated to promoting scientific discoveries and innovations in liver diseases through the publication of high-quality research papers and reviews covering various aspects of hepatology.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
