Nessmah Sultan, Mandy Foyster, Matilda Tonkovic, Danielle Noon, Helen Burton‐Murray, Jessica R. Biesiekierski, Caroline J. Tuck
{"title":"肠易激综合征患者饮食紊乱和厌食症的存在和特征","authors":"Nessmah Sultan, Mandy Foyster, Matilda Tonkovic, Danielle Noon, Helen Burton‐Murray, Jessica R. Biesiekierski, Caroline J. Tuck","doi":"10.1111/nmo.14797","DOIUrl":null,"url":null,"abstract":"IntroductionOrthorexia, a harmful obsession with eating healthily, may develop from illnesses characterized by dietary restriction, including irritable bowel syndrome (IBS) and eating disorders (ED). Evidence of disordered eating in IBS exists, but orthorexia has not been assessed. This cross‐sectional study in adults (≥18 years) assessed presence and characteristics of disordered eating and orthorexia in IBS, compared to control subjects (CS) and ED.MethodsIBS participants met Rome IV, and ED participants met DSM‐5 criteria. Disordered eating was assessed using “sick, control, one‐stone, fat, food” (SCOFF, ≥2 indicating disordered eating), and orthorexia by the eating habits questionnaire (EHQ). Secondary measures included stress (PSS); anxiety (HADS‐A); food‐related quality of life (Fr‐QoL), and dietary intake (CNAQ).Key ResultsIn 202 IBS (192 female), 34 ED (34 female), and 109 CS (90 female), more IBS (33%) and ED (47%) scored SCOFF≥2 compared to CS (16%, <jats:italic>p</jats:italic> < 0.001, chi‐square). IBS and ED had higher orthorexia symptom severity compared to CS (EHQ IBS 82.9 ± 18.1, ED 90.1 ± 19.6, and CS 73.5 ± 16.9, <jats:italic>p</jats:italic> < 0.001, one‐way ANOVA). IBS and ED did not differ for SCOFF or EHQ (<jats:italic>p</jats:italic> > 0.05). Those with IBS and disordered eating had higher orthorexia symptom severity (EHQ 78.2 ± 16.6 vs. 92.4 ± 17.5, <jats:italic>p</jats:italic> < 0.001, independent <jats:italic>t</jats:italic>‐test), worse symptoms (IBS‐SSS 211.0 ± 78.4 vs. 244.4 ± 62.5, <jats:italic>p</jats:italic> = 0.008, Mann–Whitney <jats:italic>U</jats:italic> test), higher stress (<jats:italic>p</jats:italic> < 0.001, independent <jats:italic>t</jats:italic>‐test), higher anxiety (<jats:italic>p</jats:italic> = 0.002, independent <jats:italic>t</jats:italic>‐test), and worse FR‐QoL (<jats:italic>p</jats:italic> < 0.001, independent <jats:italic>t</jats:italic>‐test).Conclusions and InferencesDisordered eating and orthorexia symptoms occur frequently in IBS, particularly in those with worse gastrointestinal symptoms, higher stress, and anxiety. Clinicians could consider these characteristics when prescribing dietary therapies.","PeriodicalId":19104,"journal":{"name":"Neurogastroenterology & Motility","volume":"99 1","pages":""},"PeriodicalIF":0.0000,"publicationDate":"2024-04-12","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"","citationCount":"0","resultStr":"{\"title\":\"Presence and characteristics of disordered eating and orthorexia in irritable bowel syndrome\",\"authors\":\"Nessmah Sultan, Mandy Foyster, Matilda Tonkovic, Danielle Noon, Helen Burton‐Murray, Jessica R. Biesiekierski, Caroline J. Tuck\",\"doi\":\"10.1111/nmo.14797\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"IntroductionOrthorexia, a harmful obsession with eating healthily, may develop from illnesses characterized by dietary restriction, including irritable bowel syndrome (IBS) and eating disorders (ED). Evidence of disordered eating in IBS exists, but orthorexia has not been assessed. This cross‐sectional study in adults (≥18 years) assessed presence and characteristics of disordered eating and orthorexia in IBS, compared to control subjects (CS) and ED.MethodsIBS participants met Rome IV, and ED participants met DSM‐5 criteria. Disordered eating was assessed using “sick, control, one‐stone, fat, food” (SCOFF, ≥2 indicating disordered eating), and orthorexia by the eating habits questionnaire (EHQ). Secondary measures included stress (PSS); anxiety (HADS‐A); food‐related quality of life (Fr‐QoL), and dietary intake (CNAQ).Key ResultsIn 202 IBS (192 female), 34 ED (34 female), and 109 CS (90 female), more IBS (33%) and ED (47%) scored SCOFF≥2 compared to CS (16%, <jats:italic>p</jats:italic> < 0.001, chi‐square). IBS and ED had higher orthorexia symptom severity compared to CS (EHQ IBS 82.9 ± 18.1, ED 90.1 ± 19.6, and CS 73.5 ± 16.9, <jats:italic>p</jats:italic> < 0.001, one‐way ANOVA). IBS and ED did not differ for SCOFF or EHQ (<jats:italic>p</jats:italic> > 0.05). Those with IBS and disordered eating had higher orthorexia symptom severity (EHQ 78.2 ± 16.6 vs. 92.4 ± 17.5, <jats:italic>p</jats:italic> < 0.001, independent <jats:italic>t</jats:italic>‐test), worse symptoms (IBS‐SSS 211.0 ± 78.4 vs. 244.4 ± 62.5, <jats:italic>p</jats:italic> = 0.008, Mann–Whitney <jats:italic>U</jats:italic> test), higher stress (<jats:italic>p</jats:italic> < 0.001, independent <jats:italic>t</jats:italic>‐test), higher anxiety (<jats:italic>p</jats:italic> = 0.002, independent <jats:italic>t</jats:italic>‐test), and worse FR‐QoL (<jats:italic>p</jats:italic> < 0.001, independent <jats:italic>t</jats:italic>‐test).Conclusions and InferencesDisordered eating and orthorexia symptoms occur frequently in IBS, particularly in those with worse gastrointestinal symptoms, higher stress, and anxiety. Clinicians could consider these characteristics when prescribing dietary therapies.\",\"PeriodicalId\":19104,\"journal\":{\"name\":\"Neurogastroenterology & Motility\",\"volume\":\"99 1\",\"pages\":\"\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2024-04-12\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Neurogastroenterology & Motility\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1111/nmo.14797\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Neurogastroenterology & Motility","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1111/nmo.14797","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
摘要
导言厌食症是一种对健康饮食有害的强迫症,可能源于以饮食限制为特征的疾病,包括肠易激综合征(IBS)和饮食失调症(ED)。有证据表明肠易激综合征患者存在饮食紊乱,但尚未对厌食症进行评估。这项横断面研究以成年人(≥18 岁)为对象,与对照组(CS)和 ED 相比,评估了 IBS 中饮食紊乱和厌食症的存在和特征。进食障碍通过 "生病、控制、一石、脂肪、食物"(SCOFF,≥2 表示进食障碍)进行评估,厌食症通过饮食习惯问卷(EHQ)进行评估。主要结果 在 202 名 IBS(192 名女性)、34 名 ED(34 名女性)和 109 名 CS(90 名女性)中,与 CS(16%,p < 0.001,chi-square)相比,更多的 IBS(33%)和 ED(47%)在 SCOFF 中得分≥2。与 CS 相比,IBS 和 ED 的厌食症状严重程度更高(EHQ IBS 82.9 ± 18.1,ED 90.1 ± 19.6,CS 73.5 ± 16.9,p < 0.001,单因素方差分析)。IBS 和 ED 在 SCOFF 或 EHQ 方面没有差异(p > 0.05)。患有肠易激综合征和进食障碍的人有较高的厌食症状严重程度(EHQ 78.2 ± 16.6 vs. 92.4 ± 17.5,p < 0.001,独立 t 检验)、较差的症状(IBS-SSS 211.0 ± 78.4 vs. 244.4 ± 62.5,p = 0.008,曼-惠特尼 U 检验)、较高的压力(p < 0.001,独立 t 检验)、更高的焦虑(p = 0.002,独立 t 检验)和更差的 FR-QoL (p < 0.001,独立 t 检验)。临床医生在开具饮食疗法处方时可考虑这些特征。
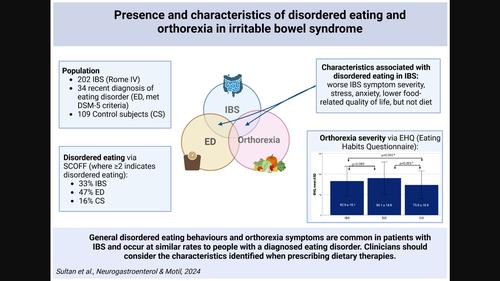
Presence and characteristics of disordered eating and orthorexia in irritable bowel syndrome
IntroductionOrthorexia, a harmful obsession with eating healthily, may develop from illnesses characterized by dietary restriction, including irritable bowel syndrome (IBS) and eating disorders (ED). Evidence of disordered eating in IBS exists, but orthorexia has not been assessed. This cross‐sectional study in adults (≥18 years) assessed presence and characteristics of disordered eating and orthorexia in IBS, compared to control subjects (CS) and ED.MethodsIBS participants met Rome IV, and ED participants met DSM‐5 criteria. Disordered eating was assessed using “sick, control, one‐stone, fat, food” (SCOFF, ≥2 indicating disordered eating), and orthorexia by the eating habits questionnaire (EHQ). Secondary measures included stress (PSS); anxiety (HADS‐A); food‐related quality of life (Fr‐QoL), and dietary intake (CNAQ).Key ResultsIn 202 IBS (192 female), 34 ED (34 female), and 109 CS (90 female), more IBS (33%) and ED (47%) scored SCOFF≥2 compared to CS (16%, p < 0.001, chi‐square). IBS and ED had higher orthorexia symptom severity compared to CS (EHQ IBS 82.9 ± 18.1, ED 90.1 ± 19.6, and CS 73.5 ± 16.9, p < 0.001, one‐way ANOVA). IBS and ED did not differ for SCOFF or EHQ (p > 0.05). Those with IBS and disordered eating had higher orthorexia symptom severity (EHQ 78.2 ± 16.6 vs. 92.4 ± 17.5, p < 0.001, independent t‐test), worse symptoms (IBS‐SSS 211.0 ± 78.4 vs. 244.4 ± 62.5, p = 0.008, Mann–Whitney U test), higher stress (p < 0.001, independent t‐test), higher anxiety (p = 0.002, independent t‐test), and worse FR‐QoL (p < 0.001, independent t‐test).Conclusions and InferencesDisordered eating and orthorexia symptoms occur frequently in IBS, particularly in those with worse gastrointestinal symptoms, higher stress, and anxiety. Clinicians could consider these characteristics when prescribing dietary therapies.



 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
