{"title":"心力衰竭--起搏器植入术后感染性心内膜炎的一个尚未探索的危险因素","authors":"","doi":"10.1016/j.jjcc.2024.04.002","DOIUrl":null,"url":null,"abstract":"<div><h3>Background</h3><p><span>With the widespread use of permanent pacemakers (PPM), and increased mortality associated with pacemaker </span>endocarditis<span>, it is essential to evaluate comorbidities that could potentially increase the risk of infective endocarditis (IE). Heart failure (HF), a common comorbidity, has not been well studied as an independent risk factor for development of IE in individuals with PPM.</span></p></div><div><h3>Methods</h3><p><span><span>The US National Inpatient Sample database was used to sample individuals with PPM. Patients with concomitant implantable cardioverter defibrillator, </span>acute heart failure<span><span>, history of endocarditis, intravenous drug use, </span>prosthetic heart valves, or central venous </span></span>catheter infection<span> were excluded. Propensity matching was performed to match patients with and without HF. Pre- and post-match logistic regression was performed to assess HF as an independent risk factor for IE. A subgroup analysis was performed comparing IE rates between patients with HF with reduced (HFrEF) vs preserved (HFpEF) ejection fraction.</span></p></div><div><h3>Results</h3><p><span>Out of 333,571 patients with PPM included in the study, 121,862 (37 %) had HF. HF patients were older and had a higher prevalence of females. All comorbidities except for dental disease and cancer were more prevalent in the HF group. Patients with HF were 1.30 times more likely to develop IE [OR: 1.30 (1.16–1.47); </span><em>p</em><span> < 0.001]. The two cohorts were then matched for age, gender, and 20 comorbidities using a 1:1 propensity score matching algorithm. After matching, HF was still independently associated with increased risk of IE [OR: 1.62 (1.36–1.93); </span><em>p</em><span> < 0.001]. In our sub-group analysis, HFrEF and HFpEF patients had similar IE rates.</span></p></div><div><h3>Conclusion</h3><p>In PPM population, HF was associated with an increased risk of IE compared to those without HF. We hypothesize that HF being a low-flow and high-inflammatory state might have contributed to this increased risk. Larger studies are required to corroborate our findings and evaluate the need for antimicrobial prophylaxis for this population.</p></div>","PeriodicalId":15223,"journal":{"name":"Journal of cardiology","volume":null,"pages":null},"PeriodicalIF":2.5000,"publicationDate":"2024-04-06","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"","citationCount":"0","resultStr":"{\"title\":\"Heart failure — An unexplored risk factor for infective endocarditis after pacemaker implantation\",\"authors\":\"\",\"doi\":\"10.1016/j.jjcc.2024.04.002\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<div><h3>Background</h3><p><span>With the widespread use of permanent pacemakers (PPM), and increased mortality associated with pacemaker </span>endocarditis<span>, it is essential to evaluate comorbidities that could potentially increase the risk of infective endocarditis (IE). Heart failure (HF), a common comorbidity, has not been well studied as an independent risk factor for development of IE in individuals with PPM.</span></p></div><div><h3>Methods</h3><p><span><span>The US National Inpatient Sample database was used to sample individuals with PPM. Patients with concomitant implantable cardioverter defibrillator, </span>acute heart failure<span><span>, history of endocarditis, intravenous drug use, </span>prosthetic heart valves, or central venous </span></span>catheter infection<span> were excluded. Propensity matching was performed to match patients with and without HF. Pre- and post-match logistic regression was performed to assess HF as an independent risk factor for IE. A subgroup analysis was performed comparing IE rates between patients with HF with reduced (HFrEF) vs preserved (HFpEF) ejection fraction.</span></p></div><div><h3>Results</h3><p><span>Out of 333,571 patients with PPM included in the study, 121,862 (37 %) had HF. HF patients were older and had a higher prevalence of females. All comorbidities except for dental disease and cancer were more prevalent in the HF group. Patients with HF were 1.30 times more likely to develop IE [OR: 1.30 (1.16–1.47); </span><em>p</em><span> < 0.001]. The two cohorts were then matched for age, gender, and 20 comorbidities using a 1:1 propensity score matching algorithm. After matching, HF was still independently associated with increased risk of IE [OR: 1.62 (1.36–1.93); </span><em>p</em><span> < 0.001]. In our sub-group analysis, HFrEF and HFpEF patients had similar IE rates.</span></p></div><div><h3>Conclusion</h3><p>In PPM population, HF was associated with an increased risk of IE compared to those without HF. We hypothesize that HF being a low-flow and high-inflammatory state might have contributed to this increased risk. Larger studies are required to corroborate our findings and evaluate the need for antimicrobial prophylaxis for this population.</p></div>\",\"PeriodicalId\":15223,\"journal\":{\"name\":\"Journal of cardiology\",\"volume\":null,\"pages\":null},\"PeriodicalIF\":2.5000,\"publicationDate\":\"2024-04-06\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of cardiology\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://www.sciencedirect.com/science/article/pii/S0914508724000613\",\"RegionNum\":3,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q2\",\"JCRName\":\"CARDIAC & CARDIOVASCULAR SYSTEMS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of cardiology","FirstCategoryId":"3","ListUrlMain":"https://www.sciencedirect.com/science/article/pii/S0914508724000613","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
Heart failure — An unexplored risk factor for infective endocarditis after pacemaker implantation
Background
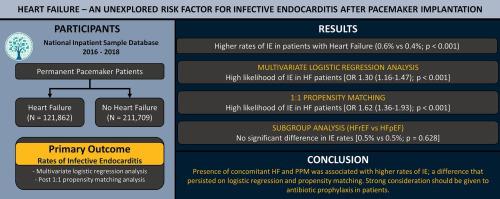
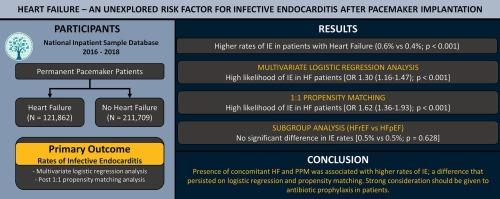
With the widespread use of permanent pacemakers (PPM), and increased mortality associated with pacemaker endocarditis, it is essential to evaluate comorbidities that could potentially increase the risk of infective endocarditis (IE). Heart failure (HF), a common comorbidity, has not been well studied as an independent risk factor for development of IE in individuals with PPM.
Methods
The US National Inpatient Sample database was used to sample individuals with PPM. Patients with concomitant implantable cardioverter defibrillator, acute heart failure, history of endocarditis, intravenous drug use, prosthetic heart valves, or central venous catheter infection were excluded. Propensity matching was performed to match patients with and without HF. Pre- and post-match logistic regression was performed to assess HF as an independent risk factor for IE. A subgroup analysis was performed comparing IE rates between patients with HF with reduced (HFrEF) vs preserved (HFpEF) ejection fraction.
Results
Out of 333,571 patients with PPM included in the study, 121,862 (37 %) had HF. HF patients were older and had a higher prevalence of females. All comorbidities except for dental disease and cancer were more prevalent in the HF group. Patients with HF were 1.30 times more likely to develop IE [OR: 1.30 (1.16–1.47); p < 0.001]. The two cohorts were then matched for age, gender, and 20 comorbidities using a 1:1 propensity score matching algorithm. After matching, HF was still independently associated with increased risk of IE [OR: 1.62 (1.36–1.93); p < 0.001]. In our sub-group analysis, HFrEF and HFpEF patients had similar IE rates.
Conclusion
In PPM population, HF was associated with an increased risk of IE compared to those without HF. We hypothesize that HF being a low-flow and high-inflammatory state might have contributed to this increased risk. Larger studies are required to corroborate our findings and evaluate the need for antimicrobial prophylaxis for this population.
期刊介绍:
The official journal of the Japanese College of Cardiology is an international, English language, peer-reviewed journal publishing the latest findings in cardiovascular medicine. Journal of Cardiology (JC) aims to publish the highest-quality material covering original basic and clinical research on all aspects of cardiovascular disease. Topics covered include ischemic heart disease, cardiomyopathy, valvular heart disease, vascular disease, hypertension, arrhythmia, congenital heart disease, pharmacological and non-pharmacological treatment, new diagnostic techniques, and cardiovascular imaging. JC also publishes a selection of review articles, clinical trials, short communications, and important messages and letters to the editor.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
