Hanjun Zhang, Mingyue Song, Mingzhan Du, Zhuxue Zhang, Weiguo Zhang
{"title":"肝实质中的原发性卡斯特曼病:病例报告和文献综述","authors":"Hanjun Zhang, Mingyue Song, Mingzhan Du, Zhuxue Zhang, Weiguo Zhang","doi":"10.1002/ird3.74","DOIUrl":null,"url":null,"abstract":"<p>A 65-year-old woman was found to have a space-occupying lesion in the parenchyma of hepatic segment IV by ultrasonography during a routine medical checkup. She had no history of viral hepatitis or any infectious diseases, and her tumor markers and routine blood and biochemical indices were normal. Gadoxetic acid-enhanced magnetic resonance imaging revealed a well-defined lesion that showed homogeneous hypointensity on T1-weighted images and hyperintensity with a halo sign on T2-weighted images (Figure 1a,b). Diffusion-weighted imaging showed homogeneous restricted diffusion (Figure 1c,d), and dynamic contrast-enhanced imaging showed hyperintensity in the arterial phase with no Gd-EOB-DTPA uptake in the hepatobiliary phase (Figure 1e–g). A maximum standardized uptake value (SUV<sub>max</sub>) of 3.270 and a delayed SUV<sub>max</sub> of 4.887 were recorded on <sup>18</sup>F-fluorodeoxyglucose positron emission tomography/computed tomography (FDG-PET/CT) scans (Figure 2a–d). The plasma cell variant of Castleman's disease was confirmed pathologically after left hemihepatectomy. Immunohistochemical analysis showed lymphoid hyperplasia, positive immunostaining for CD markers, and a Ki-67 index of 40% (Figure 2e,f). No recurrence has been noted on annual computed tomography scans after the 6-month follow-up.</p><p>Castleman's disease, also known as angiofollicular lymph node hyperplasia and giant lymph node hyperplasia [<span>1</span>], rarely arises in the hepatic parenchyma. Clinically, Castleman's disease can be divided into unicentric (UCD) and multicentric (MCD). UCD and idiopathic MCD are classified into tumor-like lesions with B-cell predominance according to the fifth edition of the World Health Organization classification of haematolymphoid tumors [<span>2, 3</span>].</p><p>UCD usually presents as a localized lesion without any obvious symptoms [<span>4</span>]. Diagnosis of hepatic UCD remains difficult because of a lack of specific imaging features. In our case, it was necessary to rule out the possibility of hemangioendothelioma in view of the presence of a halo sign on T2-weighted images. However, our patient had none of the hallmarks of hemangioendothelioma, such as the “capsular retraction” sign [<span>5</span>]. On dynamic enhanced magnetic resonance imaging, the corona-like enhancement of this lesion can be confused with hepatocellular carcinoma (HCC). Nevertheless, the lesion lacked a capsule and the classical “wash in and wash out” dynamic enhancement pattern typical of HCC [<span>6</span>].</p><p>Of note, the corona-like enhancement and the halo sign seen in our case may also be seen in hepatocellular adenoma. However, the lesion did not show the atoll sign or signal drop out on out-of-phase imaging or uptake of a hepatocyte-specific contrast agent [<span>7</span>]. Furthermore, the lesion in our case showed a low signal in the hepatobiliary phase, which rules out focal nodular hyperplasia [<span>8, 9</span>].</p><p>The lesion in our case showed remarkable hyperintensity on diffusion-weighted imaging and had an Apparent Diffusion Coefficient value of 0.850 × 10<sup>−3</sup>, which generally indicates a cell-rich lesion like lymphoma or HCC [<span>10-12</span>]. More cases need to be collected to address this relatively specific feature in the diagnosis of UCD.</p><p>The lesion in our case showed moderate metabolism on <sup>18</sup>F-FDG PET/CT with an SUV<sub>max</sub> of 3.270, which may indicate malignancy, although inflammatory or granulomatous disease such as tuberculoma or granuloma cannot be ruled out. [<span>13</span>] Although this positive finding on PET/CT in a patient with Castleman's disease has yet to be elucidated, one of the explanations may be that the cell proliferation rate is higher for UCD than for normal hepatocytes but slower than for malignant tumor cells. The phenomenon of FDG uptake in UCD lesions has been reported in literature [<span>14-17</span>]. Metastasis could be excluded in our patient because of the lack of marked glucose uptake at other sites, including lymph nodes.</p><p>In conclusion, UCD in the hepatic parenchyma is extremely rare and has no specific features, which makes preoperative diagnosis challenging for radiologists. However, certain imaging characteristics on magnetic resonance imaging, such as the halo sign, restricted diffusion, and corona-like enhancement as well as moderate metabolism on <sup>18</sup>F-FDG PET/CT may facilitate the differentiation of UCD from other hepatic conditions, which may be helpful for patient care in the clinical setting.</p><p>Hanjun Zhang analyzed the data and prepared the first draft of the manuscript. Mingyue Song participated in the conception and design of the study, Zhuxue Zhang constructively revised the manuscript; Mingzhan Du participated in data collection and organization; Weiguo Zhang participated in and supervised the study throughout, and they share corresponding authorship. All authors commented on previous versions of the manuscript and approved the final version.</p><p>The authors declare no conflicts of interest.</p><p>Not applicable.</p><p>Not applicable.</p>","PeriodicalId":73508,"journal":{"name":"iRadiology","volume":"2 4","pages":"422-425"},"PeriodicalIF":0.0000,"publicationDate":"2024-04-15","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1002/ird3.74","citationCount":"0","resultStr":"{\"title\":\"Primary Castleman's disease in the hepatic parenchyma: A case report and literature review\",\"authors\":\"Hanjun Zhang, Mingyue Song, Mingzhan Du, Zhuxue Zhang, Weiguo Zhang\",\"doi\":\"10.1002/ird3.74\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p>A 65-year-old woman was found to have a space-occupying lesion in the parenchyma of hepatic segment IV by ultrasonography during a routine medical checkup. She had no history of viral hepatitis or any infectious diseases, and her tumor markers and routine blood and biochemical indices were normal. Gadoxetic acid-enhanced magnetic resonance imaging revealed a well-defined lesion that showed homogeneous hypointensity on T1-weighted images and hyperintensity with a halo sign on T2-weighted images (Figure 1a,b). Diffusion-weighted imaging showed homogeneous restricted diffusion (Figure 1c,d), and dynamic contrast-enhanced imaging showed hyperintensity in the arterial phase with no Gd-EOB-DTPA uptake in the hepatobiliary phase (Figure 1e–g). A maximum standardized uptake value (SUV<sub>max</sub>) of 3.270 and a delayed SUV<sub>max</sub> of 4.887 were recorded on <sup>18</sup>F-fluorodeoxyglucose positron emission tomography/computed tomography (FDG-PET/CT) scans (Figure 2a–d). The plasma cell variant of Castleman's disease was confirmed pathologically after left hemihepatectomy. Immunohistochemical analysis showed lymphoid hyperplasia, positive immunostaining for CD markers, and a Ki-67 index of 40% (Figure 2e,f). No recurrence has been noted on annual computed tomography scans after the 6-month follow-up.</p><p>Castleman's disease, also known as angiofollicular lymph node hyperplasia and giant lymph node hyperplasia [<span>1</span>], rarely arises in the hepatic parenchyma. Clinically, Castleman's disease can be divided into unicentric (UCD) and multicentric (MCD). UCD and idiopathic MCD are classified into tumor-like lesions with B-cell predominance according to the fifth edition of the World Health Organization classification of haematolymphoid tumors [<span>2, 3</span>].</p><p>UCD usually presents as a localized lesion without any obvious symptoms [<span>4</span>]. Diagnosis of hepatic UCD remains difficult because of a lack of specific imaging features. In our case, it was necessary to rule out the possibility of hemangioendothelioma in view of the presence of a halo sign on T2-weighted images. However, our patient had none of the hallmarks of hemangioendothelioma, such as the “capsular retraction” sign [<span>5</span>]. On dynamic enhanced magnetic resonance imaging, the corona-like enhancement of this lesion can be confused with hepatocellular carcinoma (HCC). Nevertheless, the lesion lacked a capsule and the classical “wash in and wash out” dynamic enhancement pattern typical of HCC [<span>6</span>].</p><p>Of note, the corona-like enhancement and the halo sign seen in our case may also be seen in hepatocellular adenoma. However, the lesion did not show the atoll sign or signal drop out on out-of-phase imaging or uptake of a hepatocyte-specific contrast agent [<span>7</span>]. Furthermore, the lesion in our case showed a low signal in the hepatobiliary phase, which rules out focal nodular hyperplasia [<span>8, 9</span>].</p><p>The lesion in our case showed remarkable hyperintensity on diffusion-weighted imaging and had an Apparent Diffusion Coefficient value of 0.850 × 10<sup>−3</sup>, which generally indicates a cell-rich lesion like lymphoma or HCC [<span>10-12</span>]. More cases need to be collected to address this relatively specific feature in the diagnosis of UCD.</p><p>The lesion in our case showed moderate metabolism on <sup>18</sup>F-FDG PET/CT with an SUV<sub>max</sub> of 3.270, which may indicate malignancy, although inflammatory or granulomatous disease such as tuberculoma or granuloma cannot be ruled out. [<span>13</span>] Although this positive finding on PET/CT in a patient with Castleman's disease has yet to be elucidated, one of the explanations may be that the cell proliferation rate is higher for UCD than for normal hepatocytes but slower than for malignant tumor cells. The phenomenon of FDG uptake in UCD lesions has been reported in literature [<span>14-17</span>]. Metastasis could be excluded in our patient because of the lack of marked glucose uptake at other sites, including lymph nodes.</p><p>In conclusion, UCD in the hepatic parenchyma is extremely rare and has no specific features, which makes preoperative diagnosis challenging for radiologists. However, certain imaging characteristics on magnetic resonance imaging, such as the halo sign, restricted diffusion, and corona-like enhancement as well as moderate metabolism on <sup>18</sup>F-FDG PET/CT may facilitate the differentiation of UCD from other hepatic conditions, which may be helpful for patient care in the clinical setting.</p><p>Hanjun Zhang analyzed the data and prepared the first draft of the manuscript. Mingyue Song participated in the conception and design of the study, Zhuxue Zhang constructively revised the manuscript; Mingzhan Du participated in data collection and organization; Weiguo Zhang participated in and supervised the study throughout, and they share corresponding authorship. All authors commented on previous versions of the manuscript and approved the final version.</p><p>The authors declare no conflicts of interest.</p><p>Not applicable.</p><p>Not applicable.</p>\",\"PeriodicalId\":73508,\"journal\":{\"name\":\"iRadiology\",\"volume\":\"2 4\",\"pages\":\"422-425\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2024-04-15\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://onlinelibrary.wiley.com/doi/epdf/10.1002/ird3.74\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"iRadiology\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://onlinelibrary.wiley.com/doi/10.1002/ird3.74\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"iRadiology","FirstCategoryId":"1085","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1002/ird3.74","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
Primary Castleman's disease in the hepatic parenchyma: A case report and literature review
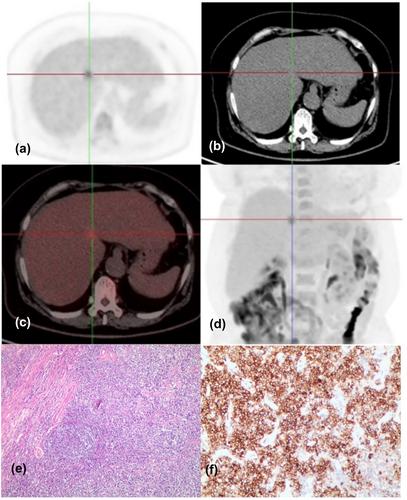
A 65-year-old woman was found to have a space-occupying lesion in the parenchyma of hepatic segment IV by ultrasonography during a routine medical checkup. She had no history of viral hepatitis or any infectious diseases, and her tumor markers and routine blood and biochemical indices were normal. Gadoxetic acid-enhanced magnetic resonance imaging revealed a well-defined lesion that showed homogeneous hypointensity on T1-weighted images and hyperintensity with a halo sign on T2-weighted images (Figure 1a,b). Diffusion-weighted imaging showed homogeneous restricted diffusion (Figure 1c,d), and dynamic contrast-enhanced imaging showed hyperintensity in the arterial phase with no Gd-EOB-DTPA uptake in the hepatobiliary phase (Figure 1e–g). A maximum standardized uptake value (SUVmax) of 3.270 and a delayed SUVmax of 4.887 were recorded on 18F-fluorodeoxyglucose positron emission tomography/computed tomography (FDG-PET/CT) scans (Figure 2a–d). The plasma cell variant of Castleman's disease was confirmed pathologically after left hemihepatectomy. Immunohistochemical analysis showed lymphoid hyperplasia, positive immunostaining for CD markers, and a Ki-67 index of 40% (Figure 2e,f). No recurrence has been noted on annual computed tomography scans after the 6-month follow-up.
Castleman's disease, also known as angiofollicular lymph node hyperplasia and giant lymph node hyperplasia [1], rarely arises in the hepatic parenchyma. Clinically, Castleman's disease can be divided into unicentric (UCD) and multicentric (MCD). UCD and idiopathic MCD are classified into tumor-like lesions with B-cell predominance according to the fifth edition of the World Health Organization classification of haematolymphoid tumors [2, 3].
UCD usually presents as a localized lesion without any obvious symptoms [4]. Diagnosis of hepatic UCD remains difficult because of a lack of specific imaging features. In our case, it was necessary to rule out the possibility of hemangioendothelioma in view of the presence of a halo sign on T2-weighted images. However, our patient had none of the hallmarks of hemangioendothelioma, such as the “capsular retraction” sign [5]. On dynamic enhanced magnetic resonance imaging, the corona-like enhancement of this lesion can be confused with hepatocellular carcinoma (HCC). Nevertheless, the lesion lacked a capsule and the classical “wash in and wash out” dynamic enhancement pattern typical of HCC [6].
Of note, the corona-like enhancement and the halo sign seen in our case may also be seen in hepatocellular adenoma. However, the lesion did not show the atoll sign or signal drop out on out-of-phase imaging or uptake of a hepatocyte-specific contrast agent [7]. Furthermore, the lesion in our case showed a low signal in the hepatobiliary phase, which rules out focal nodular hyperplasia [8, 9].
The lesion in our case showed remarkable hyperintensity on diffusion-weighted imaging and had an Apparent Diffusion Coefficient value of 0.850 × 10−3, which generally indicates a cell-rich lesion like lymphoma or HCC [10-12]. More cases need to be collected to address this relatively specific feature in the diagnosis of UCD.
The lesion in our case showed moderate metabolism on 18F-FDG PET/CT with an SUVmax of 3.270, which may indicate malignancy, although inflammatory or granulomatous disease such as tuberculoma or granuloma cannot be ruled out. [13] Although this positive finding on PET/CT in a patient with Castleman's disease has yet to be elucidated, one of the explanations may be that the cell proliferation rate is higher for UCD than for normal hepatocytes but slower than for malignant tumor cells. The phenomenon of FDG uptake in UCD lesions has been reported in literature [14-17]. Metastasis could be excluded in our patient because of the lack of marked glucose uptake at other sites, including lymph nodes.
In conclusion, UCD in the hepatic parenchyma is extremely rare and has no specific features, which makes preoperative diagnosis challenging for radiologists. However, certain imaging characteristics on magnetic resonance imaging, such as the halo sign, restricted diffusion, and corona-like enhancement as well as moderate metabolism on 18F-FDG PET/CT may facilitate the differentiation of UCD from other hepatic conditions, which may be helpful for patient care in the clinical setting.
Hanjun Zhang analyzed the data and prepared the first draft of the manuscript. Mingyue Song participated in the conception and design of the study, Zhuxue Zhang constructively revised the manuscript; Mingzhan Du participated in data collection and organization; Weiguo Zhang participated in and supervised the study throughout, and they share corresponding authorship. All authors commented on previous versions of the manuscript and approved the final version.


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
