{"title":"用于筛查胎盘早剥谱的临床声像图评分:系统回顾和荟萃分析。","authors":"","doi":"10.1016/j.ajogmf.2024.101369","DOIUrl":null,"url":null,"abstract":"<div><h3>OBJECTIVE</h3><p><span>Clinical-sonographic scoring systems combining clinical features and ultrasound imaging markers have been proposed for the screening of </span>placenta accreta<span> spectrum, but their usefulness in different settings remains limited. This study aimed to assess and compare different clinical-sonographic score systems applied from mid-pregnancy for the prenatal evaluation of patients at risk of placenta accreta spectrum at birth.</span></p></div><div><h3>DATA SOURCES</h3><p>PubMed/MEDLINE, Google Scholar, and Embase were searched between October 1982 and October 2022 to identify eligible studies.</p></div><div><h3>STUDY ELIGIBILITY CRITERIA</h3><p>Observational studies providing data on the use of a combined clinical-ultrasound score system applied from mid-pregnancy for the prenatal evaluation of placenta accreta spectrum were included.</p></div><div><h3>METHODS</h3><p>Study characteristics were evaluated by 2 independent reviewers using a predesigned protocol registered on PROSPERO (CRD42022332486). Heterogeneity among studies was analyzed with Cochran's Q-test and I<sup>2</sup> statistics. Statistical heterogeneity was quantified by estimating the variance between the studies using I<sup>2</sup> statistics. The area under the receiver operating characteristic curve of each score and their summary receiver operating characteristic curves were calculated with sensitivity and specificity, and the integrated score of the summaries of the receiver operating characteristic curves of all sonographic markers was calculated. Forest plots were used to develop the meta-analysis of each sonographic marker and for the integrated sonographic score.</p></div><div><h3>RESULTS</h3><p>Of 1028 articles reviewed, 12 cohorts and 2 case–control studies including 1630 patients screened for placenta accreta spectrum by clinical-ultrasound scores met the eligibility criteria. A diagnosis of placenta accreta spectrum was reported in 602 (36.9%) cases, for which 547 (90.9%) intraoperative findings and/or histopathologic data were described. A wide variation was observed among the studies in reported sensitivities and specificities and in thresholds used for the identification of patients with a high probability of placenta accreta spectrum at birth. The summaries of the areas under the curve of the individual sonographic scores ranged from 0.85 (the lowest) for subplacental hypervascularity to 0.91 for placental location in the lower uterine segment, myometrial thinning, and placental lacunae and 0.95 for the loss of clear zone. Only 4 studies included placental bulging in their sonographic score system, and therefore no meta-analysis for this score was performed. The integrated summary of the areas under the curve was 0.83 (95% confidence interval, 79–0.86). Forest plot analysis revealed integrated sensitivities and specificities of 0.68 (95% confidence interval, 0.53–0.80) and 0.88 (95% confidence interval, 0.68–0.96), respectively.</p></div><div><h3>CONCLUSION</h3><p><span>Clinical-sonographic score systems can contribute to the prenatal screening of patients at risk of placenta accreta spectrum at birth. Although we included multiple sonographic studies conducted during the mid-pregnancy period, standardized evaluation should be performed not only with strict ultrasound criteria for the placental position, mid </span>third trimester<span> gestational age at examination, and sonographic markers associated with PAS. Numeric sensitivities, specificities, NPVs, PPV, LR-, and LR+ should be recorded prospectively to assess their accuracy in different set-ups and PTP should be verified at delivery. The variables recommended for most predictive screening are: loss of clear zone underneath the placental bed, placentation in the LUS, and placenta lacunae.</span></p></div>","PeriodicalId":36186,"journal":{"name":"American Journal of Obstetrics & Gynecology Mfm","volume":"6 8","pages":"Article 101369"},"PeriodicalIF":3.1000,"publicationDate":"2024-08-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"","citationCount":"0","resultStr":"{\"title\":\"Clinical-sonographic scores for the screening of placenta accreta spectrum: a systematic review and meta-analysis\",\"authors\":\"\",\"doi\":\"10.1016/j.ajogmf.2024.101369\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<div><h3>OBJECTIVE</h3><p><span>Clinical-sonographic scoring systems combining clinical features and ultrasound imaging markers have been proposed for the screening of </span>placenta accreta<span> spectrum, but their usefulness in different settings remains limited. This study aimed to assess and compare different clinical-sonographic score systems applied from mid-pregnancy for the prenatal evaluation of patients at risk of placenta accreta spectrum at birth.</span></p></div><div><h3>DATA SOURCES</h3><p>PubMed/MEDLINE, Google Scholar, and Embase were searched between October 1982 and October 2022 to identify eligible studies.</p></div><div><h3>STUDY ELIGIBILITY CRITERIA</h3><p>Observational studies providing data on the use of a combined clinical-ultrasound score system applied from mid-pregnancy for the prenatal evaluation of placenta accreta spectrum were included.</p></div><div><h3>METHODS</h3><p>Study characteristics were evaluated by 2 independent reviewers using a predesigned protocol registered on PROSPERO (CRD42022332486). Heterogeneity among studies was analyzed with Cochran's Q-test and I<sup>2</sup> statistics. Statistical heterogeneity was quantified by estimating the variance between the studies using I<sup>2</sup> statistics. The area under the receiver operating characteristic curve of each score and their summary receiver operating characteristic curves were calculated with sensitivity and specificity, and the integrated score of the summaries of the receiver operating characteristic curves of all sonographic markers was calculated. Forest plots were used to develop the meta-analysis of each sonographic marker and for the integrated sonographic score.</p></div><div><h3>RESULTS</h3><p>Of 1028 articles reviewed, 12 cohorts and 2 case–control studies including 1630 patients screened for placenta accreta spectrum by clinical-ultrasound scores met the eligibility criteria. A diagnosis of placenta accreta spectrum was reported in 602 (36.9%) cases, for which 547 (90.9%) intraoperative findings and/or histopathologic data were described. A wide variation was observed among the studies in reported sensitivities and specificities and in thresholds used for the identification of patients with a high probability of placenta accreta spectrum at birth. The summaries of the areas under the curve of the individual sonographic scores ranged from 0.85 (the lowest) for subplacental hypervascularity to 0.91 for placental location in the lower uterine segment, myometrial thinning, and placental lacunae and 0.95 for the loss of clear zone. Only 4 studies included placental bulging in their sonographic score system, and therefore no meta-analysis for this score was performed. The integrated summary of the areas under the curve was 0.83 (95% confidence interval, 79–0.86). Forest plot analysis revealed integrated sensitivities and specificities of 0.68 (95% confidence interval, 0.53–0.80) and 0.88 (95% confidence interval, 0.68–0.96), respectively.</p></div><div><h3>CONCLUSION</h3><p><span>Clinical-sonographic score systems can contribute to the prenatal screening of patients at risk of placenta accreta spectrum at birth. Although we included multiple sonographic studies conducted during the mid-pregnancy period, standardized evaluation should be performed not only with strict ultrasound criteria for the placental position, mid </span>third trimester<span> gestational age at examination, and sonographic markers associated with PAS. Numeric sensitivities, specificities, NPVs, PPV, LR-, and LR+ should be recorded prospectively to assess their accuracy in different set-ups and PTP should be verified at delivery. The variables recommended for most predictive screening are: loss of clear zone underneath the placental bed, placentation in the LUS, and placenta lacunae.</span></p></div>\",\"PeriodicalId\":36186,\"journal\":{\"name\":\"American Journal of Obstetrics & Gynecology Mfm\",\"volume\":\"6 8\",\"pages\":\"Article 101369\"},\"PeriodicalIF\":3.1000,\"publicationDate\":\"2024-08-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"American Journal of Obstetrics & Gynecology Mfm\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://www.sciencedirect.com/science/article/pii/S2589933324000958\",\"RegionNum\":2,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2024/4/16 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q1\",\"JCRName\":\"OBSTETRICS & GYNECOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"American Journal of Obstetrics & Gynecology Mfm","FirstCategoryId":"3","ListUrlMain":"https://www.sciencedirect.com/science/article/pii/S2589933324000958","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/4/16 0:00:00","PubModel":"Epub","JCR":"Q1","JCRName":"OBSTETRICS & GYNECOLOGY","Score":null,"Total":0}
Clinical-sonographic scores for the screening of placenta accreta spectrum: a systematic review and meta-analysis
OBJECTIVE
Clinical-sonographic scoring systems combining clinical features and ultrasound imaging markers have been proposed for the screening of placenta accreta spectrum, but their usefulness in different settings remains limited. This study aimed to assess and compare different clinical-sonographic score systems applied from mid-pregnancy for the prenatal evaluation of patients at risk of placenta accreta spectrum at birth.
DATA SOURCES
PubMed/MEDLINE, Google Scholar, and Embase were searched between October 1982 and October 2022 to identify eligible studies.
STUDY ELIGIBILITY CRITERIA
Observational studies providing data on the use of a combined clinical-ultrasound score system applied from mid-pregnancy for the prenatal evaluation of placenta accreta spectrum were included.
METHODS
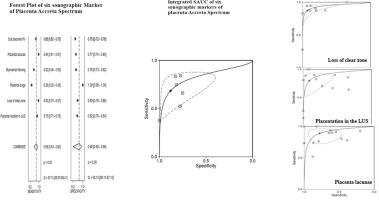
Study characteristics were evaluated by 2 independent reviewers using a predesigned protocol registered on PROSPERO (CRD42022332486). Heterogeneity among studies was analyzed with Cochran's Q-test and I2 statistics. Statistical heterogeneity was quantified by estimating the variance between the studies using I2 statistics. The area under the receiver operating characteristic curve of each score and their summary receiver operating characteristic curves were calculated with sensitivity and specificity, and the integrated score of the summaries of the receiver operating characteristic curves of all sonographic markers was calculated. Forest plots were used to develop the meta-analysis of each sonographic marker and for the integrated sonographic score.
RESULTS
Of 1028 articles reviewed, 12 cohorts and 2 case–control studies including 1630 patients screened for placenta accreta spectrum by clinical-ultrasound scores met the eligibility criteria. A diagnosis of placenta accreta spectrum was reported in 602 (36.9%) cases, for which 547 (90.9%) intraoperative findings and/or histopathologic data were described. A wide variation was observed among the studies in reported sensitivities and specificities and in thresholds used for the identification of patients with a high probability of placenta accreta spectrum at birth. The summaries of the areas under the curve of the individual sonographic scores ranged from 0.85 (the lowest) for subplacental hypervascularity to 0.91 for placental location in the lower uterine segment, myometrial thinning, and placental lacunae and 0.95 for the loss of clear zone. Only 4 studies included placental bulging in their sonographic score system, and therefore no meta-analysis for this score was performed. The integrated summary of the areas under the curve was 0.83 (95% confidence interval, 79–0.86). Forest plot analysis revealed integrated sensitivities and specificities of 0.68 (95% confidence interval, 0.53–0.80) and 0.88 (95% confidence interval, 0.68–0.96), respectively.
CONCLUSION
Clinical-sonographic score systems can contribute to the prenatal screening of patients at risk of placenta accreta spectrum at birth. Although we included multiple sonographic studies conducted during the mid-pregnancy period, standardized evaluation should be performed not only with strict ultrasound criteria for the placental position, mid third trimester gestational age at examination, and sonographic markers associated with PAS. Numeric sensitivities, specificities, NPVs, PPV, LR-, and LR+ should be recorded prospectively to assess their accuracy in different set-ups and PTP should be verified at delivery. The variables recommended for most predictive screening are: loss of clear zone underneath the placental bed, placentation in the LUS, and placenta lacunae.
期刊介绍:
The American Journal of Obstetrics and Gynecology (AJOG) is a highly esteemed publication with two companion titles. One of these is the American Journal of Obstetrics and Gynecology Maternal-Fetal Medicine (AJOG MFM), which is dedicated to the latest research in the field of maternal-fetal medicine, specifically concerning high-risk pregnancies. The journal encompasses a wide range of topics, including:
Maternal Complications: It addresses significant studies that have the potential to change clinical practice regarding complications faced by pregnant women.
Fetal Complications: The journal covers prenatal diagnosis, ultrasound, and genetic issues related to the fetus, providing insights into the management and care of fetal health.
Prenatal Care: It discusses the best practices in prenatal care to ensure the health and well-being of both the mother and the unborn child.
Intrapartum Care: It provides guidance on the care provided during the childbirth process, which is critical for the safety of both mother and baby.
Postpartum Issues: The journal also tackles issues that arise after childbirth, focusing on the postpartum period and its implications for maternal health. AJOG MFM serves as a reliable forum for peer-reviewed research, with a preference for randomized trials and meta-analyses. The goal is to equip researchers and clinicians with the most current information and evidence-based strategies to effectively manage high-risk pregnancies and to provide the best possible care for mothers and their unborn children.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
