May Hagiwara, Victoria Divino, Swapna Munnangi, Mark Delegge, Suna Park, Ed G Marins, Kaili Ren, Charlie Strange
{"title":"α-1抗胰蛋白酶缺乏症合并肝脏和/或肺部疾病患者的医疗资源利用率和成本:美国的一项纵向回顾性研究。","authors":"May Hagiwara, Victoria Divino, Swapna Munnangi, Mark Delegge, Suna Park, Ed G Marins, Kaili Ren, Charlie Strange","doi":"10.57264/cer-2023-0186","DOIUrl":null,"url":null,"abstract":"<p><p><b>Aim:</b> To evaluate all-cause and liver-associated healthcare resource utilization (HCRU) and costs among patients with alpha-1 antitrypsin deficiency (AATD) with liver disease (LD) and/or lung disease (LgD). <b>Materials & methods:</b> This was a retrospective analysis of linked administrative claims data from the IQVIA PharMetrics<sup>®</sup> Plus and the IQVIA Ambulatory Electronic Medical Records (AEMR) databases from 1 July 2021 to 31 January 2022. Patients with AATD in the IQVIA PharMetrics Plus database were included with ≥1 inpatient or ≥2 outpatient medical claims ≥90 days apart with a diagnosis of AATD, or with records indicating a protease inhibitor (Pi)*ZZ/Pi*MZ genotype in the IQVIA AEMR database with linkage to IQVIA PharMetrics Plus. For a patient's identified continuous enrollment period, patient time was assigned to health states based on the initial encounter with an LD/LgD diagnosis. A unique index date was defined for each health state, and HCRU and costs were calculated per person-year (PPY). <b>Results:</b> Overall, 5136 adult and pediatric patients from the IQVIA PharMetrics Plus and IQVIA AEMR databases were analyzed. All-cause and liver-associated HCRU and costs were substantially higher following onset of LD/LgD. All-cause cost PPY ranged from US $11,877 in the absence of either LD/LgD to US $74,015 in the presence of both LD and LgD. Among liver transplant recipients in the AATD with LD health state, liver-associated total costs PPY were US $87,329 1-year pre-transplantation and US $461,752 1-year post-transplantation. In the AATD with LgD and AATD with LD and LgD health states, patients who received augmentation therapy were associated with higher all-cause total costs PPY and lower liver-associated total costs PPY than their counterparts who did not receive augmentation therapy. <b>Conclusion:</b> Patients with AATD had increased HCRU and healthcare costs in the presence of LD and/or LgD. HCRU and healthcare costs were highest in the AATD with LD and LgD health state.</p>","PeriodicalId":15539,"journal":{"name":"Journal of comparative effectiveness research","volume":" ","pages":"e230186"},"PeriodicalIF":2.5000,"publicationDate":"2024-06-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11145523/pdf/","citationCount":"0","resultStr":"{\"title\":\"Healthcare resource utilization and costs among patients with alpha-1 antitrypsin deficiency with liver and/or lung disease: a longitudinal retrospective study in the USA.\",\"authors\":\"May Hagiwara, Victoria Divino, Swapna Munnangi, Mark Delegge, Suna Park, Ed G Marins, Kaili Ren, Charlie Strange\",\"doi\":\"10.57264/cer-2023-0186\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p><b>Aim:</b> To evaluate all-cause and liver-associated healthcare resource utilization (HCRU) and costs among patients with alpha-1 antitrypsin deficiency (AATD) with liver disease (LD) and/or lung disease (LgD). <b>Materials & methods:</b> This was a retrospective analysis of linked administrative claims data from the IQVIA PharMetrics<sup>®</sup> Plus and the IQVIA Ambulatory Electronic Medical Records (AEMR) databases from 1 July 2021 to 31 January 2022. Patients with AATD in the IQVIA PharMetrics Plus database were included with ≥1 inpatient or ≥2 outpatient medical claims ≥90 days apart with a diagnosis of AATD, or with records indicating a protease inhibitor (Pi)*ZZ/Pi*MZ genotype in the IQVIA AEMR database with linkage to IQVIA PharMetrics Plus. For a patient's identified continuous enrollment period, patient time was assigned to health states based on the initial encounter with an LD/LgD diagnosis. A unique index date was defined for each health state, and HCRU and costs were calculated per person-year (PPY). <b>Results:</b> Overall, 5136 adult and pediatric patients from the IQVIA PharMetrics Plus and IQVIA AEMR databases were analyzed. All-cause and liver-associated HCRU and costs were substantially higher following onset of LD/LgD. All-cause cost PPY ranged from US $11,877 in the absence of either LD/LgD to US $74,015 in the presence of both LD and LgD. Among liver transplant recipients in the AATD with LD health state, liver-associated total costs PPY were US $87,329 1-year pre-transplantation and US $461,752 1-year post-transplantation. In the AATD with LgD and AATD with LD and LgD health states, patients who received augmentation therapy were associated with higher all-cause total costs PPY and lower liver-associated total costs PPY than their counterparts who did not receive augmentation therapy. <b>Conclusion:</b> Patients with AATD had increased HCRU and healthcare costs in the presence of LD and/or LgD. HCRU and healthcare costs were highest in the AATD with LD and LgD health state.</p>\",\"PeriodicalId\":15539,\"journal\":{\"name\":\"Journal of comparative effectiveness research\",\"volume\":\" \",\"pages\":\"e230186\"},\"PeriodicalIF\":2.5000,\"publicationDate\":\"2024-06-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11145523/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of comparative effectiveness research\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.57264/cer-2023-0186\",\"RegionNum\":4,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2024/5/2 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q3\",\"JCRName\":\"HEALTH CARE SCIENCES & SERVICES\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of comparative effectiveness research","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.57264/cer-2023-0186","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/5/2 0:00:00","PubModel":"Epub","JCR":"Q3","JCRName":"HEALTH CARE SCIENCES & SERVICES","Score":null,"Total":0}
Healthcare resource utilization and costs among patients with alpha-1 antitrypsin deficiency with liver and/or lung disease: a longitudinal retrospective study in the USA.
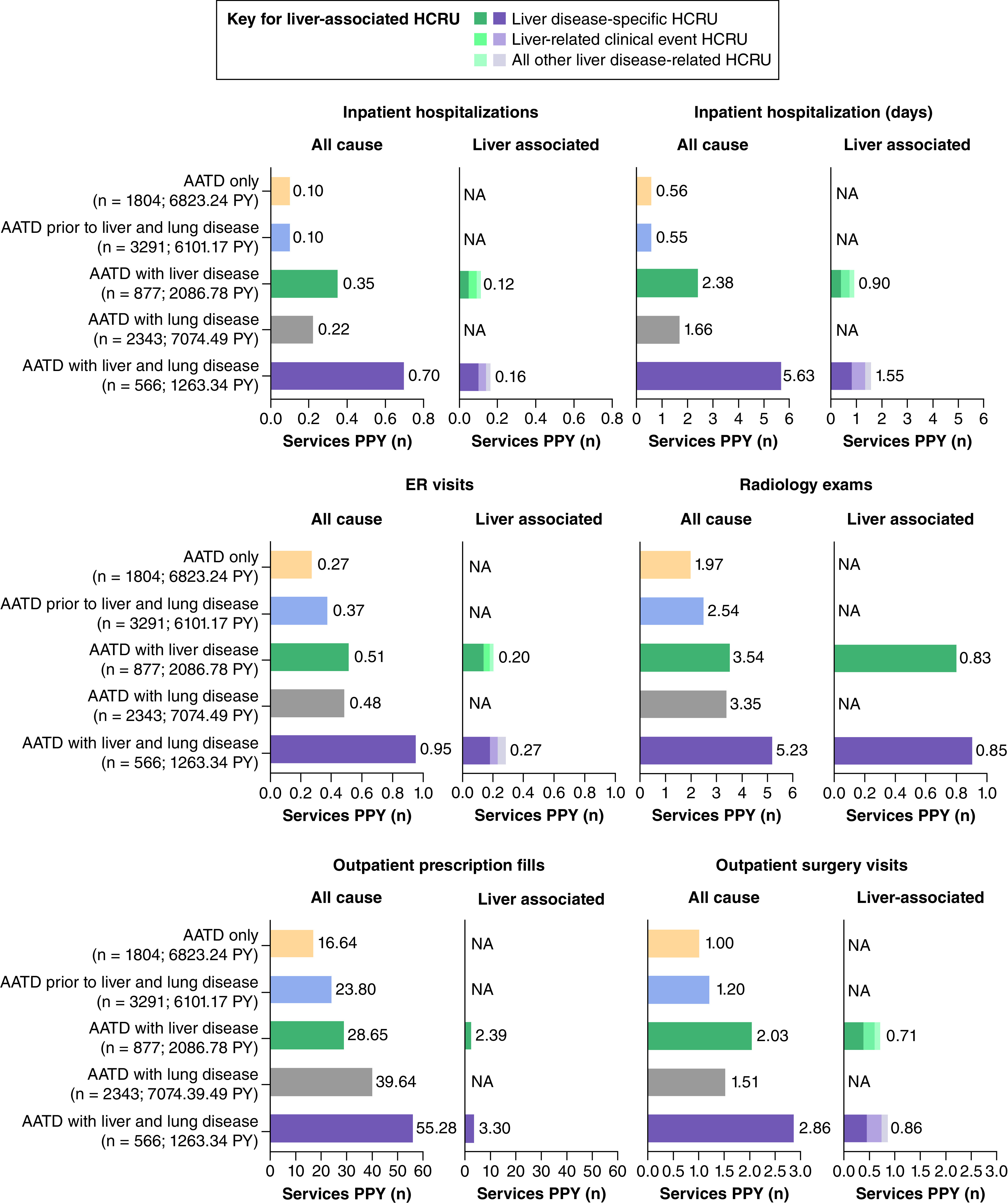
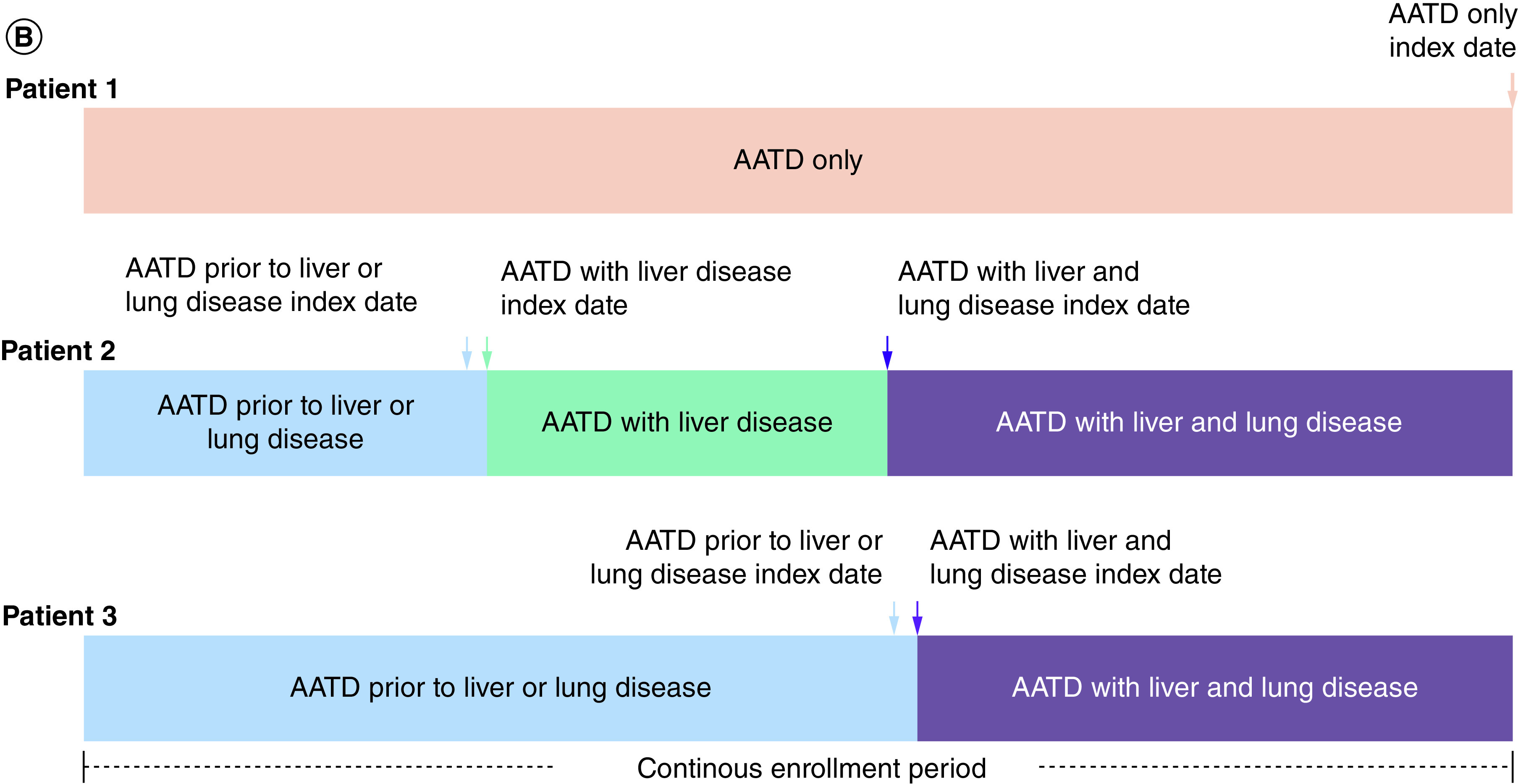
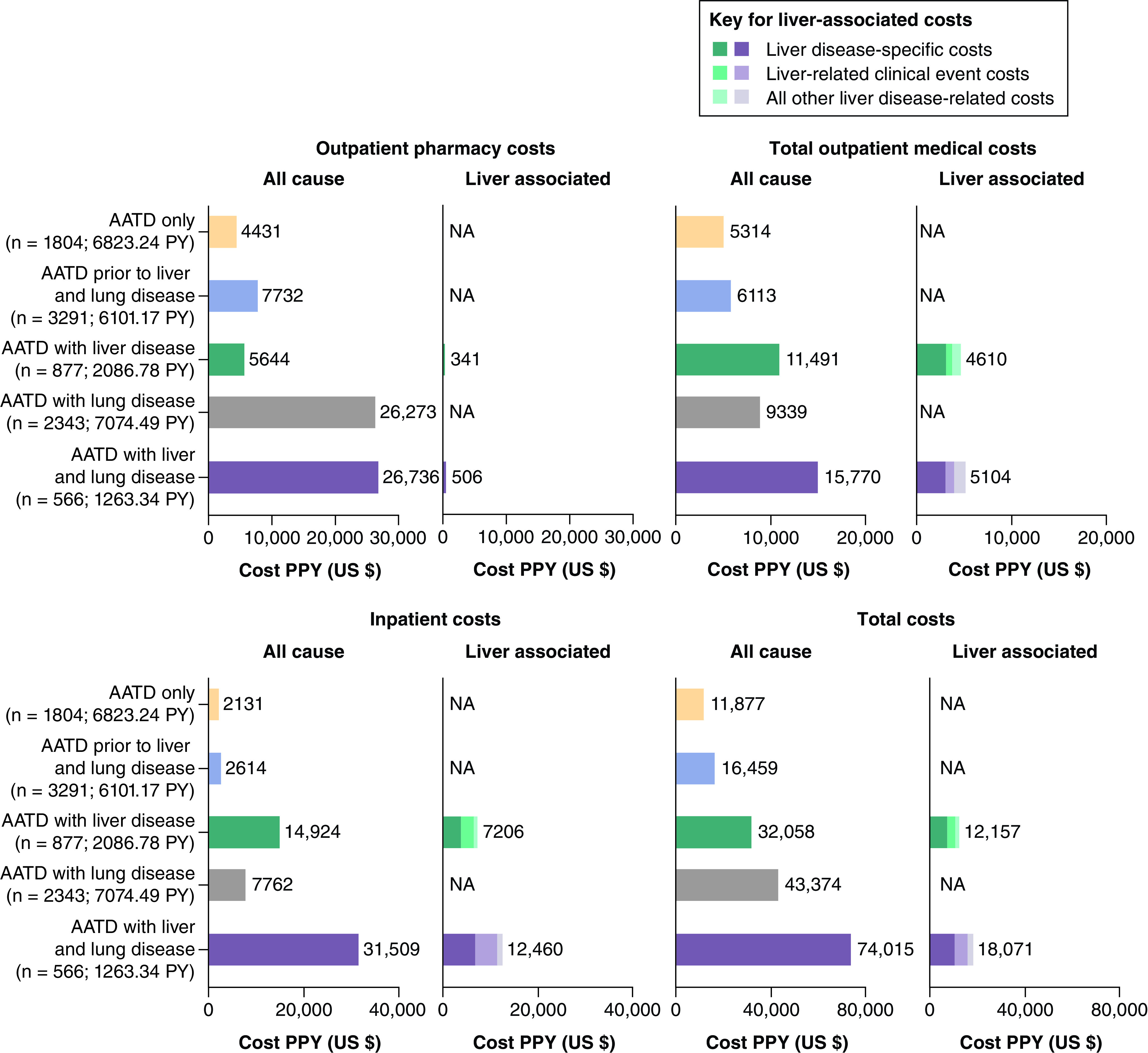
Aim: To evaluate all-cause and liver-associated healthcare resource utilization (HCRU) and costs among patients with alpha-1 antitrypsin deficiency (AATD) with liver disease (LD) and/or lung disease (LgD). Materials & methods: This was a retrospective analysis of linked administrative claims data from the IQVIA PharMetrics® Plus and the IQVIA Ambulatory Electronic Medical Records (AEMR) databases from 1 July 2021 to 31 January 2022. Patients with AATD in the IQVIA PharMetrics Plus database were included with ≥1 inpatient or ≥2 outpatient medical claims ≥90 days apart with a diagnosis of AATD, or with records indicating a protease inhibitor (Pi)*ZZ/Pi*MZ genotype in the IQVIA AEMR database with linkage to IQVIA PharMetrics Plus. For a patient's identified continuous enrollment period, patient time was assigned to health states based on the initial encounter with an LD/LgD diagnosis. A unique index date was defined for each health state, and HCRU and costs were calculated per person-year (PPY). Results: Overall, 5136 adult and pediatric patients from the IQVIA PharMetrics Plus and IQVIA AEMR databases were analyzed. All-cause and liver-associated HCRU and costs were substantially higher following onset of LD/LgD. All-cause cost PPY ranged from US $11,877 in the absence of either LD/LgD to US $74,015 in the presence of both LD and LgD. Among liver transplant recipients in the AATD with LD health state, liver-associated total costs PPY were US $87,329 1-year pre-transplantation and US $461,752 1-year post-transplantation. In the AATD with LgD and AATD with LD and LgD health states, patients who received augmentation therapy were associated with higher all-cause total costs PPY and lower liver-associated total costs PPY than their counterparts who did not receive augmentation therapy. Conclusion: Patients with AATD had increased HCRU and healthcare costs in the presence of LD and/or LgD. HCRU and healthcare costs were highest in the AATD with LD and LgD health state.
期刊介绍:
Journal of Comparative Effectiveness Research provides a rapid-publication platform for debate, and for the presentation of new findings and research methodologies.
Through rigorous evaluation and comprehensive coverage, the Journal of Comparative Effectiveness Research provides stakeholders (including patients, clinicians, healthcare purchasers, and health policy makers) with the key data and opinions to make informed and specific decisions on clinical practice.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
