Michael M Covell, Joanna M Roy, Nithin Gupta, Ahmed Sami Raihane, Kranti C Rumalla, Amanda Cyntia Lima Fonseca Rodrigues, Evan Courville, Christian A Bowers
{"title":"颅内脑膜瘤切除术中的虚弱情况:风险分析指数在预测非居家出院和住院死亡率方面显示出很强的辨别能力。","authors":"Michael M Covell, Joanna M Roy, Nithin Gupta, Ahmed Sami Raihane, Kranti C Rumalla, Amanda Cyntia Lima Fonseca Rodrigues, Evan Courville, Christian A Bowers","doi":"10.1007/s11060-024-04703-5","DOIUrl":null,"url":null,"abstract":"<p><strong>Purpose: </strong>Frailty is an independent risk factor for adverse postoperative outcomes following intracranial meningioma resection (IMR). The role of the Risk Analysis Index (RAI) in predicting postoperative outcomes following IMR is nascent but may inform preoperative patient selection and surgical planning.</p><p><strong>Methods: </strong>IMR patients from the Nationwide Inpatient Sample were identified using diagnostic and procedural codes (2019-2020). The relationship between preoperative RAI-measured frailty and primary outcomes (non-home discharge (NHD), in-hospital mortality) and secondary outcomes (extended length of stay (eLOS), complication rates) was assessed via multivariate analyses. The discriminatory accuracy of the RAI for primary outcomes was measured in area under the receiver operating characteristic (AUROC) curve analysis.</p><p><strong>Results: </strong>A total of 23,230 IMR patients (mean age = 59) were identified, with frailty statuses stratified by RAI score: 0-20 \"robust\" (R)(N = 10,665, 45.9%), 21-30 \"normal\" (N)(N = 8,895, 38.3%), 31-40 \"frail\" (F)(N = 2,605, 11.2%), and 41+ \"very frail\" (VF)(N = 1,065, 4.6%). Rates of NHD (R 11.5%, N 29.7%, F 60.8%, VF 61.5%), in-hospital mortality (R 0.5%, N 1.8%, F 3.8%, VF 7.0%), eLOS (R 13.2%, N 21.5%, F 40.9%, VF 46.0%), and complications (R 7.5%, N 11.6%, F 15.7%, VF 16.0%) significantly increased with increasing frailty thresholds (p < 0.001). The RAI demonstrated strong discrimination for NHD (C-statistic: 0.755) and in-hospital mortality (C-statistic: 0.754) in AUROC curve analysis.</p><p><strong>Conclusion: </strong>Increasing RAI-measured frailty is significantly associated with increased complication rates, eLOS, NHD, and in-hospital mortality following IMR. The RAI demonstrates strong discrimination for predicting NHD and in-hospital mortality following IMR, and may aid in preoperative risk stratification.</p>","PeriodicalId":16425,"journal":{"name":"Journal of Neuro-Oncology","volume":" ","pages":"85-93"},"PeriodicalIF":3.4000,"publicationDate":"2024-08-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"","citationCount":"0","resultStr":"{\"title\":\"Frailty in intracranial meningioma resection: the risk analysis index demonstrates strong discrimination for predicting non-home discharge and in-hospital mortality.\",\"authors\":\"Michael M Covell, Joanna M Roy, Nithin Gupta, Ahmed Sami Raihane, Kranti C Rumalla, Amanda Cyntia Lima Fonseca Rodrigues, Evan Courville, Christian A Bowers\",\"doi\":\"10.1007/s11060-024-04703-5\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Purpose: </strong>Frailty is an independent risk factor for adverse postoperative outcomes following intracranial meningioma resection (IMR). The role of the Risk Analysis Index (RAI) in predicting postoperative outcomes following IMR is nascent but may inform preoperative patient selection and surgical planning.</p><p><strong>Methods: </strong>IMR patients from the Nationwide Inpatient Sample were identified using diagnostic and procedural codes (2019-2020). The relationship between preoperative RAI-measured frailty and primary outcomes (non-home discharge (NHD), in-hospital mortality) and secondary outcomes (extended length of stay (eLOS), complication rates) was assessed via multivariate analyses. The discriminatory accuracy of the RAI for primary outcomes was measured in area under the receiver operating characteristic (AUROC) curve analysis.</p><p><strong>Results: </strong>A total of 23,230 IMR patients (mean age = 59) were identified, with frailty statuses stratified by RAI score: 0-20 \\\"robust\\\" (R)(N = 10,665, 45.9%), 21-30 \\\"normal\\\" (N)(N = 8,895, 38.3%), 31-40 \\\"frail\\\" (F)(N = 2,605, 11.2%), and 41+ \\\"very frail\\\" (VF)(N = 1,065, 4.6%). Rates of NHD (R 11.5%, N 29.7%, F 60.8%, VF 61.5%), in-hospital mortality (R 0.5%, N 1.8%, F 3.8%, VF 7.0%), eLOS (R 13.2%, N 21.5%, F 40.9%, VF 46.0%), and complications (R 7.5%, N 11.6%, F 15.7%, VF 16.0%) significantly increased with increasing frailty thresholds (p < 0.001). The RAI demonstrated strong discrimination for NHD (C-statistic: 0.755) and in-hospital mortality (C-statistic: 0.754) in AUROC curve analysis.</p><p><strong>Conclusion: </strong>Increasing RAI-measured frailty is significantly associated with increased complication rates, eLOS, NHD, and in-hospital mortality following IMR. The RAI demonstrates strong discrimination for predicting NHD and in-hospital mortality following IMR, and may aid in preoperative risk stratification.</p>\",\"PeriodicalId\":16425,\"journal\":{\"name\":\"Journal of Neuro-Oncology\",\"volume\":\" \",\"pages\":\"85-93\"},\"PeriodicalIF\":3.4000,\"publicationDate\":\"2024-08-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of Neuro-Oncology\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1007/s11060-024-04703-5\",\"RegionNum\":2,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2024/5/7 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q2\",\"JCRName\":\"CLINICAL NEUROLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Neuro-Oncology","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1007/s11060-024-04703-5","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/5/7 0:00:00","PubModel":"Epub","JCR":"Q2","JCRName":"CLINICAL NEUROLOGY","Score":null,"Total":0}
Frailty in intracranial meningioma resection: the risk analysis index demonstrates strong discrimination for predicting non-home discharge and in-hospital mortality.
Purpose: Frailty is an independent risk factor for adverse postoperative outcomes following intracranial meningioma resection (IMR). The role of the Risk Analysis Index (RAI) in predicting postoperative outcomes following IMR is nascent but may inform preoperative patient selection and surgical planning.
Methods: IMR patients from the Nationwide Inpatient Sample were identified using diagnostic and procedural codes (2019-2020). The relationship between preoperative RAI-measured frailty and primary outcomes (non-home discharge (NHD), in-hospital mortality) and secondary outcomes (extended length of stay (eLOS), complication rates) was assessed via multivariate analyses. The discriminatory accuracy of the RAI for primary outcomes was measured in area under the receiver operating characteristic (AUROC) curve analysis.
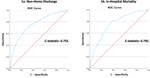
Results: A total of 23,230 IMR patients (mean age = 59) were identified, with frailty statuses stratified by RAI score: 0-20 "robust" (R)(N = 10,665, 45.9%), 21-30 "normal" (N)(N = 8,895, 38.3%), 31-40 "frail" (F)(N = 2,605, 11.2%), and 41+ "very frail" (VF)(N = 1,065, 4.6%). Rates of NHD (R 11.5%, N 29.7%, F 60.8%, VF 61.5%), in-hospital mortality (R 0.5%, N 1.8%, F 3.8%, VF 7.0%), eLOS (R 13.2%, N 21.5%, F 40.9%, VF 46.0%), and complications (R 7.5%, N 11.6%, F 15.7%, VF 16.0%) significantly increased with increasing frailty thresholds (p < 0.001). The RAI demonstrated strong discrimination for NHD (C-statistic: 0.755) and in-hospital mortality (C-statistic: 0.754) in AUROC curve analysis.
Conclusion: Increasing RAI-measured frailty is significantly associated with increased complication rates, eLOS, NHD, and in-hospital mortality following IMR. The RAI demonstrates strong discrimination for predicting NHD and in-hospital mortality following IMR, and may aid in preoperative risk stratification.
期刊介绍:
The Journal of Neuro-Oncology is a multi-disciplinary journal encompassing basic, applied, and clinical investigations in all research areas as they relate to cancer and the central nervous system. It provides a single forum for communication among neurologists, neurosurgeons, radiotherapists, medical oncologists, neuropathologists, neurodiagnosticians, and laboratory-based oncologists conducting relevant research. The Journal of Neuro-Oncology does not seek to isolate the field, but rather to focus the efforts of many disciplines in one publication through a format which pulls together these diverse interests. More than any other field of oncology, cancer of the central nervous system requires multi-disciplinary approaches. To alleviate having to scan dozens of journals of cell biology, pathology, laboratory and clinical endeavours, JNO is a periodical in which current, high-quality, relevant research in all aspects of neuro-oncology may be found.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
