Macarena C García, Lauren M Rossen, Kevin Matthews, Gery Guy, Katrina F Trivers, Cheryll C Thomas, Linda Schieb, Michael F Iademarco
{"title":"2010-2022 年美国非大都市和大都市郡五大主要死因中可预防的过早死亡。","authors":"Macarena C García, Lauren M Rossen, Kevin Matthews, Gery Guy, Katrina F Trivers, Cheryll C Thomas, Linda Schieb, Michael F Iademarco","doi":"10.15585/mmwr.ss7302a1","DOIUrl":null,"url":null,"abstract":"<p><strong>Problem/condition: </strong>A 2019 report quantified the higher percentage of potentially excess (preventable) deaths in U.S. nonmetropolitan areas compared with metropolitan areas during 2010-2017. In that report, CDC compared national, regional, and state estimates of preventable premature deaths from the five leading causes of death in nonmetropolitan and metropolitan counties during 2010-2017. This report provides estimates of preventable premature deaths for additional years (2010-2022).</p><p><strong>Period covered: </strong>2010-2022.</p><p><strong>Description of system: </strong>Mortality data for U.S. residents from the National Vital Statistics System were used to calculate preventable premature deaths from the five leading causes of death among persons aged <80 years. CDC's National Center for Health Statistics urban-rural classification scheme for counties was used to categorize the deaths according to the urban-rural county classification level of the decedent's county of residence (1: large central metropolitan [most urban], 2: large fringe metropolitan, 3: medium metropolitan, 4: small metropolitan, 5: micropolitan, and 6: noncore [most rural]). Preventable premature deaths were defined as deaths among persons aged <80 years that exceeded the number expected if the death rates for each cause in all states were equivalent to those in the benchmark states (i.e., the three states with the lowest rates). Preventable premature deaths were calculated separately for the six urban-rural county categories nationally, the 10 U.S. Department of Health and Human Services public health regions, and the 50 states and the District of Columbia.</p><p><strong>Results: </strong>During 2010-2022, the percentage of preventable premature deaths among persons aged <80 years in the United States increased for unintentional injury (e.g., unintentional poisoning including drug overdose, unintentional motor vehicle traffic crash, unintentional drowning, and unintentional fall) and stroke, decreased for cancer and chronic lower respiratory disease (CLRD), and remained stable for heart disease. The percentages of preventable premature deaths from the five leading causes of death were higher in rural counties in all years during 2010-2022. When assessed by the six urban-rural county classifications, percentages of preventable premature deaths in the most rural counties (noncore) were consistently higher than in the most urban counties (large central metropolitan and fringe metropolitan) for the five leading causes of death during the study period.During 2010-2022, preventable premature deaths from heart disease increased most in noncore (+9.5%) and micropolitan counties (+9.1%) and decreased most in large central metropolitan counties (-10.2%). Preventable premature deaths from cancer decreased in all county categories, with the largest decreases in large central metropolitan and large fringe metropolitan counties (-100.0%; benchmark achieved in both county categories in 2019). In all county categories, preventable premature deaths from unintentional injury increased, with the largest increases occurring in large central metropolitan (+147.5%) and large fringe metropolitan (+97.5%) counties. Preventable premature deaths from CLRD decreased most in large central metropolitan counties where the benchmark was achieved in 2019 and increased slightly in noncore counties (+0.8%). In all county categories, preventable premature deaths from stroke decreased from 2010 to 2013, remained constant from 2013 to 2019, and then increased in 2020 at the start of the COVID-19 pandemic. Percentages of preventable premature deaths varied across states by urban-rural county classification during 2010-2022.</p><p><strong>Interpretation: </strong>During 2010-2022, nonmetropolitan counties had higher percentages of preventable premature deaths from the five leading causes of death than did metropolitan counties nationwide, across public health regions, and in most states. The gap between the most rural and most urban counties for preventable premature deaths increased during 2010-2022 for four causes of death (cancer, heart disease, CLRD, and stroke) and decreased for unintentional injury. Urban and suburban counties (large central metropolitan, large fringe metropolitan, medium metropolitan, and small metropolitan) experienced increases in preventable premature deaths from unintentional injury during 2010-2022, leading to a narrower gap between the already high (approximately 69% in 2022) percentage of preventable premature deaths in noncore and micropolitan counties. Sharp increases in preventable premature deaths from unintentional injury, heart disease, and stroke were observed in 2020, whereas preventable premature deaths from CLRD and cancer continued to decline. CLRD deaths decreased during 2017-2020 but increased in 2022. An increase in the percentage of preventable premature deaths for multiple leading causes of death was observed in 2020 and was likely associated with COVID-19-related conditions that contributed to increased mortality from heart disease and stroke.</p><p><strong>Public health action: </strong>Routine tracking of preventable premature deaths based on urban-rural county classification might enable public health departments to identify and monitor geographic disparities in health outcomes. These disparities might be related to different levels of access to health care, social determinants of health, and other risk factors. Identifying areas with a high prevalence of potentially preventable mortality might be informative for interventions.</p>","PeriodicalId":48549,"journal":{"name":"Mmwr Surveillance Summaries","volume":"73 2","pages":"1-11"},"PeriodicalIF":49.8000,"publicationDate":"2024-05-02","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11065459/pdf/","citationCount":"0","resultStr":"{\"title\":\"Preventable Premature Deaths from the Five Leading Causes of Death in Nonmetropolitan and Metropolitan Counties, United States, 2010-2022.\",\"authors\":\"Macarena C García, Lauren M Rossen, Kevin Matthews, Gery Guy, Katrina F Trivers, Cheryll C Thomas, Linda Schieb, Michael F Iademarco\",\"doi\":\"10.15585/mmwr.ss7302a1\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Problem/condition: </strong>A 2019 report quantified the higher percentage of potentially excess (preventable) deaths in U.S. nonmetropolitan areas compared with metropolitan areas during 2010-2017. In that report, CDC compared national, regional, and state estimates of preventable premature deaths from the five leading causes of death in nonmetropolitan and metropolitan counties during 2010-2017. This report provides estimates of preventable premature deaths for additional years (2010-2022).</p><p><strong>Period covered: </strong>2010-2022.</p><p><strong>Description of system: </strong>Mortality data for U.S. residents from the National Vital Statistics System were used to calculate preventable premature deaths from the five leading causes of death among persons aged <80 years. CDC's National Center for Health Statistics urban-rural classification scheme for counties was used to categorize the deaths according to the urban-rural county classification level of the decedent's county of residence (1: large central metropolitan [most urban], 2: large fringe metropolitan, 3: medium metropolitan, 4: small metropolitan, 5: micropolitan, and 6: noncore [most rural]). Preventable premature deaths were defined as deaths among persons aged <80 years that exceeded the number expected if the death rates for each cause in all states were equivalent to those in the benchmark states (i.e., the three states with the lowest rates). Preventable premature deaths were calculated separately for the six urban-rural county categories nationally, the 10 U.S. Department of Health and Human Services public health regions, and the 50 states and the District of Columbia.</p><p><strong>Results: </strong>During 2010-2022, the percentage of preventable premature deaths among persons aged <80 years in the United States increased for unintentional injury (e.g., unintentional poisoning including drug overdose, unintentional motor vehicle traffic crash, unintentional drowning, and unintentional fall) and stroke, decreased for cancer and chronic lower respiratory disease (CLRD), and remained stable for heart disease. The percentages of preventable premature deaths from the five leading causes of death were higher in rural counties in all years during 2010-2022. When assessed by the six urban-rural county classifications, percentages of preventable premature deaths in the most rural counties (noncore) were consistently higher than in the most urban counties (large central metropolitan and fringe metropolitan) for the five leading causes of death during the study period.During 2010-2022, preventable premature deaths from heart disease increased most in noncore (+9.5%) and micropolitan counties (+9.1%) and decreased most in large central metropolitan counties (-10.2%). Preventable premature deaths from cancer decreased in all county categories, with the largest decreases in large central metropolitan and large fringe metropolitan counties (-100.0%; benchmark achieved in both county categories in 2019). In all county categories, preventable premature deaths from unintentional injury increased, with the largest increases occurring in large central metropolitan (+147.5%) and large fringe metropolitan (+97.5%) counties. Preventable premature deaths from CLRD decreased most in large central metropolitan counties where the benchmark was achieved in 2019 and increased slightly in noncore counties (+0.8%). In all county categories, preventable premature deaths from stroke decreased from 2010 to 2013, remained constant from 2013 to 2019, and then increased in 2020 at the start of the COVID-19 pandemic. Percentages of preventable premature deaths varied across states by urban-rural county classification during 2010-2022.</p><p><strong>Interpretation: </strong>During 2010-2022, nonmetropolitan counties had higher percentages of preventable premature deaths from the five leading causes of death than did metropolitan counties nationwide, across public health regions, and in most states. The gap between the most rural and most urban counties for preventable premature deaths increased during 2010-2022 for four causes of death (cancer, heart disease, CLRD, and stroke) and decreased for unintentional injury. Urban and suburban counties (large central metropolitan, large fringe metropolitan, medium metropolitan, and small metropolitan) experienced increases in preventable premature deaths from unintentional injury during 2010-2022, leading to a narrower gap between the already high (approximately 69% in 2022) percentage of preventable premature deaths in noncore and micropolitan counties. Sharp increases in preventable premature deaths from unintentional injury, heart disease, and stroke were observed in 2020, whereas preventable premature deaths from CLRD and cancer continued to decline. CLRD deaths decreased during 2017-2020 but increased in 2022. An increase in the percentage of preventable premature deaths for multiple leading causes of death was observed in 2020 and was likely associated with COVID-19-related conditions that contributed to increased mortality from heart disease and stroke.</p><p><strong>Public health action: </strong>Routine tracking of preventable premature deaths based on urban-rural county classification might enable public health departments to identify and monitor geographic disparities in health outcomes. These disparities might be related to different levels of access to health care, social determinants of health, and other risk factors. Identifying areas with a high prevalence of potentially preventable mortality might be informative for interventions.</p>\",\"PeriodicalId\":48549,\"journal\":{\"name\":\"Mmwr Surveillance Summaries\",\"volume\":\"73 2\",\"pages\":\"1-11\"},\"PeriodicalIF\":49.8000,\"publicationDate\":\"2024-05-02\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11065459/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Mmwr Surveillance Summaries\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.15585/mmwr.ss7302a1\",\"RegionNum\":1,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q1\",\"JCRName\":\"PUBLIC, ENVIRONMENTAL & OCCUPATIONAL HEALTH\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Mmwr Surveillance Summaries","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.15585/mmwr.ss7302a1","RegionNum":1,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"PUBLIC, ENVIRONMENTAL & OCCUPATIONAL HEALTH","Score":null,"Total":0}
Preventable Premature Deaths from the Five Leading Causes of Death in Nonmetropolitan and Metropolitan Counties, United States, 2010-2022.
Problem/condition: A 2019 report quantified the higher percentage of potentially excess (preventable) deaths in U.S. nonmetropolitan areas compared with metropolitan areas during 2010-2017. In that report, CDC compared national, regional, and state estimates of preventable premature deaths from the five leading causes of death in nonmetropolitan and metropolitan counties during 2010-2017. This report provides estimates of preventable premature deaths for additional years (2010-2022).
Period covered: 2010-2022.
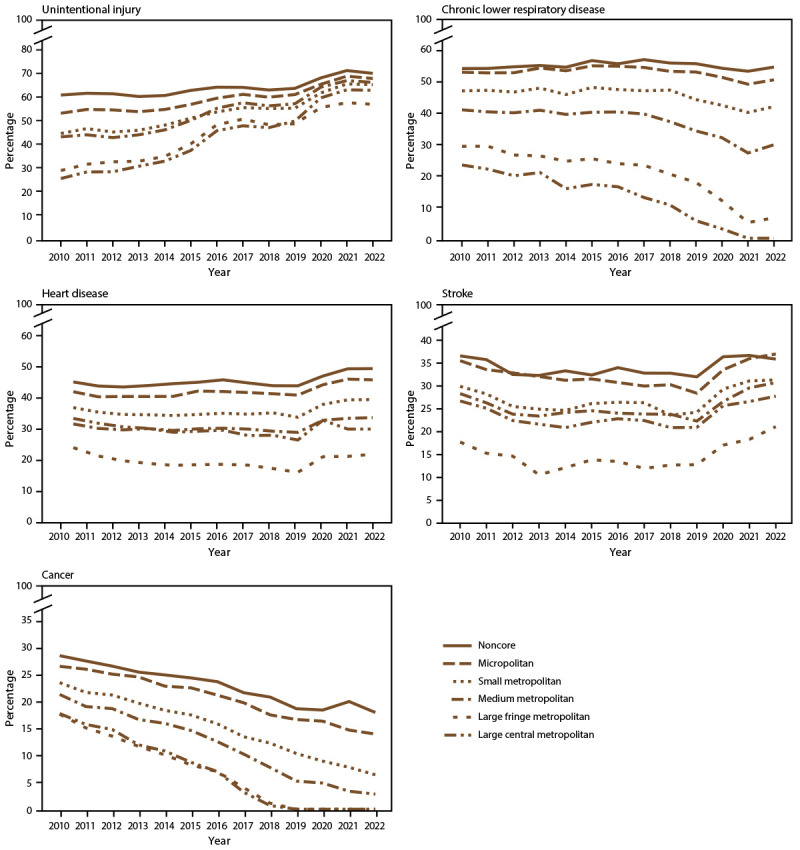
Description of system: Mortality data for U.S. residents from the National Vital Statistics System were used to calculate preventable premature deaths from the five leading causes of death among persons aged <80 years. CDC's National Center for Health Statistics urban-rural classification scheme for counties was used to categorize the deaths according to the urban-rural county classification level of the decedent's county of residence (1: large central metropolitan [most urban], 2: large fringe metropolitan, 3: medium metropolitan, 4: small metropolitan, 5: micropolitan, and 6: noncore [most rural]). Preventable premature deaths were defined as deaths among persons aged <80 years that exceeded the number expected if the death rates for each cause in all states were equivalent to those in the benchmark states (i.e., the three states with the lowest rates). Preventable premature deaths were calculated separately for the six urban-rural county categories nationally, the 10 U.S. Department of Health and Human Services public health regions, and the 50 states and the District of Columbia.
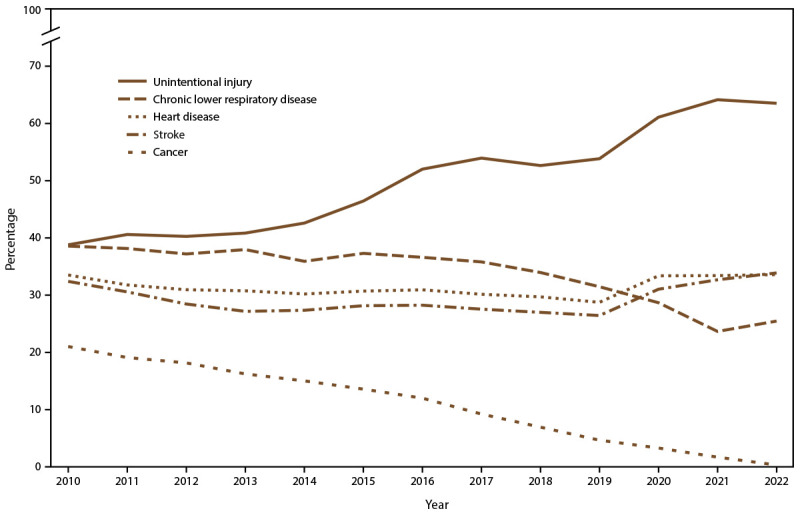
Results: During 2010-2022, the percentage of preventable premature deaths among persons aged <80 years in the United States increased for unintentional injury (e.g., unintentional poisoning including drug overdose, unintentional motor vehicle traffic crash, unintentional drowning, and unintentional fall) and stroke, decreased for cancer and chronic lower respiratory disease (CLRD), and remained stable for heart disease. The percentages of preventable premature deaths from the five leading causes of death were higher in rural counties in all years during 2010-2022. When assessed by the six urban-rural county classifications, percentages of preventable premature deaths in the most rural counties (noncore) were consistently higher than in the most urban counties (large central metropolitan and fringe metropolitan) for the five leading causes of death during the study period.During 2010-2022, preventable premature deaths from heart disease increased most in noncore (+9.5%) and micropolitan counties (+9.1%) and decreased most in large central metropolitan counties (-10.2%). Preventable premature deaths from cancer decreased in all county categories, with the largest decreases in large central metropolitan and large fringe metropolitan counties (-100.0%; benchmark achieved in both county categories in 2019). In all county categories, preventable premature deaths from unintentional injury increased, with the largest increases occurring in large central metropolitan (+147.5%) and large fringe metropolitan (+97.5%) counties. Preventable premature deaths from CLRD decreased most in large central metropolitan counties where the benchmark was achieved in 2019 and increased slightly in noncore counties (+0.8%). In all county categories, preventable premature deaths from stroke decreased from 2010 to 2013, remained constant from 2013 to 2019, and then increased in 2020 at the start of the COVID-19 pandemic. Percentages of preventable premature deaths varied across states by urban-rural county classification during 2010-2022.
Interpretation: During 2010-2022, nonmetropolitan counties had higher percentages of preventable premature deaths from the five leading causes of death than did metropolitan counties nationwide, across public health regions, and in most states. The gap between the most rural and most urban counties for preventable premature deaths increased during 2010-2022 for four causes of death (cancer, heart disease, CLRD, and stroke) and decreased for unintentional injury. Urban and suburban counties (large central metropolitan, large fringe metropolitan, medium metropolitan, and small metropolitan) experienced increases in preventable premature deaths from unintentional injury during 2010-2022, leading to a narrower gap between the already high (approximately 69% in 2022) percentage of preventable premature deaths in noncore and micropolitan counties. Sharp increases in preventable premature deaths from unintentional injury, heart disease, and stroke were observed in 2020, whereas preventable premature deaths from CLRD and cancer continued to decline. CLRD deaths decreased during 2017-2020 but increased in 2022. An increase in the percentage of preventable premature deaths for multiple leading causes of death was observed in 2020 and was likely associated with COVID-19-related conditions that contributed to increased mortality from heart disease and stroke.
Public health action: Routine tracking of preventable premature deaths based on urban-rural county classification might enable public health departments to identify and monitor geographic disparities in health outcomes. These disparities might be related to different levels of access to health care, social determinants of health, and other risk factors. Identifying areas with a high prevalence of potentially preventable mortality might be informative for interventions.
期刊介绍:
The Morbidity and Mortality Weekly Report (MMWR) Series, produced by the Centers for Disease Control and Prevention (CDC), is commonly referred to as "the voice of CDC." Serving as the primary outlet for timely, reliable, authoritative, accurate, objective, and practical public health information and recommendations, the MMWR is a crucial publication. Its readership primarily includes physicians, nurses, public health practitioners, epidemiologists, scientists, researchers, educators, and laboratorians.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
