R Scott McClure, Kenton L Rommens, Eric J Herget, Michelle Keir, Alex J Gregory, Holly N Smith, Randy D Moore
{"title":"管理远端弓、胸降主动脉和胸腹主动脉的主动脉团队模式:3 年后的评估。","authors":"R Scott McClure, Kenton L Rommens, Eric J Herget, Michelle Keir, Alex J Gregory, Holly N Smith, Randy D Moore","doi":"10.1055/s-0044-1779249","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong> This study aimed to assess feasibility, logistical challenges, and clinical outcomes associated with the implementation of an Aortic Team model for the management of distal arch, descending thoracic and thoracoabdominal aortic disease.</p><p><strong>Methods: </strong> An Aortic Team care pathway was implemented in November 2019. Working as a unit, two cardiac surgeons, two vascular surgeons, an interventional radiologist, a cardiologist, and an anesthesiologist collectively determined care decisions via multispecialty presence at an Aortic Clinic. Cardiac and vascular surgeons operated in tandem for open procedures. Interventional radiology participated alongside cardiac and vascular for endovascular procedures. Cardiology aided in medical therapies for heritable and degenerative disease, and had a lead role for genetics and high-risk pregnancy referrals. The model spanned three hospitals. Clinical outcomes at 3 years were assessed.</p><p><strong>Results: </strong> There were 35 descending thoracic and thoracoabdominal surgeries and 77 thoracic endovascular aortic repairs. Endoarch devices were used in 7 cases (Gore Thoracic Branch Endoprosthesis, 4, Terumo RelayBranch, 3) and an endothoracoabdominal device in 4 cases (Cook Zenith t-branch). The Aortic Clinic acquired 456 patients, with yearly increases (54 patients [year 1], 181 patients [year 2], 221 patients [year 3]). For surgery, mortality was 8.6% (3/35), permanent paralysis 5.7% (2/35), stroke 8.6% (3/35), permanent dialysis 0%, and reinterventions 8.6% (3/35). For endovascular cases, mortality was 3.9% (3/77), permanent paralysis 3.9% (3/77), stroke 5.2% (4/77), permanent dialysis 1.3% (1/77), and reinterventions 16.9% (13/77).</p><p><strong>Conclusion: </strong> An Aortic Team model is feasible and ensures all treatment options are considered. Conventional open thoracoabdominal procedures showed acceptable outcomes. Endoarch technology shows early promise.</p>","PeriodicalId":52392,"journal":{"name":"AORTA","volume":" ","pages":"165-173"},"PeriodicalIF":0.0000,"publicationDate":"2023-12-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11219130/pdf/","citationCount":"0","resultStr":"{\"title\":\"The Aortic Team Model for the Management of the Distal Arch, Descending Thoracic and Thoracoabdominal Aorta: Appraisal at 3 Years.\",\"authors\":\"R Scott McClure, Kenton L Rommens, Eric J Herget, Michelle Keir, Alex J Gregory, Holly N Smith, Randy D Moore\",\"doi\":\"10.1055/s-0044-1779249\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong> This study aimed to assess feasibility, logistical challenges, and clinical outcomes associated with the implementation of an Aortic Team model for the management of distal arch, descending thoracic and thoracoabdominal aortic disease.</p><p><strong>Methods: </strong> An Aortic Team care pathway was implemented in November 2019. Working as a unit, two cardiac surgeons, two vascular surgeons, an interventional radiologist, a cardiologist, and an anesthesiologist collectively determined care decisions via multispecialty presence at an Aortic Clinic. Cardiac and vascular surgeons operated in tandem for open procedures. Interventional radiology participated alongside cardiac and vascular for endovascular procedures. Cardiology aided in medical therapies for heritable and degenerative disease, and had a lead role for genetics and high-risk pregnancy referrals. The model spanned three hospitals. Clinical outcomes at 3 years were assessed.</p><p><strong>Results: </strong> There were 35 descending thoracic and thoracoabdominal surgeries and 77 thoracic endovascular aortic repairs. Endoarch devices were used in 7 cases (Gore Thoracic Branch Endoprosthesis, 4, Terumo RelayBranch, 3) and an endothoracoabdominal device in 4 cases (Cook Zenith t-branch). The Aortic Clinic acquired 456 patients, with yearly increases (54 patients [year 1], 181 patients [year 2], 221 patients [year 3]). For surgery, mortality was 8.6% (3/35), permanent paralysis 5.7% (2/35), stroke 8.6% (3/35), permanent dialysis 0%, and reinterventions 8.6% (3/35). For endovascular cases, mortality was 3.9% (3/77), permanent paralysis 3.9% (3/77), stroke 5.2% (4/77), permanent dialysis 1.3% (1/77), and reinterventions 16.9% (13/77).</p><p><strong>Conclusion: </strong> An Aortic Team model is feasible and ensures all treatment options are considered. Conventional open thoracoabdominal procedures showed acceptable outcomes. Endoarch technology shows early promise.</p>\",\"PeriodicalId\":52392,\"journal\":{\"name\":\"AORTA\",\"volume\":\" \",\"pages\":\"165-173\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2023-12-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11219130/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"AORTA\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1055/s-0044-1779249\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2024/5/2 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q3\",\"JCRName\":\"Medicine\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"AORTA","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1055/s-0044-1779249","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/5/2 0:00:00","PubModel":"Epub","JCR":"Q3","JCRName":"Medicine","Score":null,"Total":0}
The Aortic Team Model for the Management of the Distal Arch, Descending Thoracic and Thoracoabdominal Aorta: Appraisal at 3 Years.
Background: This study aimed to assess feasibility, logistical challenges, and clinical outcomes associated with the implementation of an Aortic Team model for the management of distal arch, descending thoracic and thoracoabdominal aortic disease.
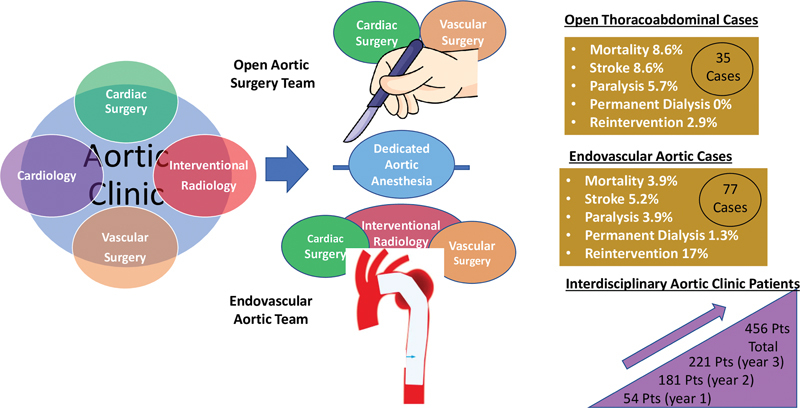
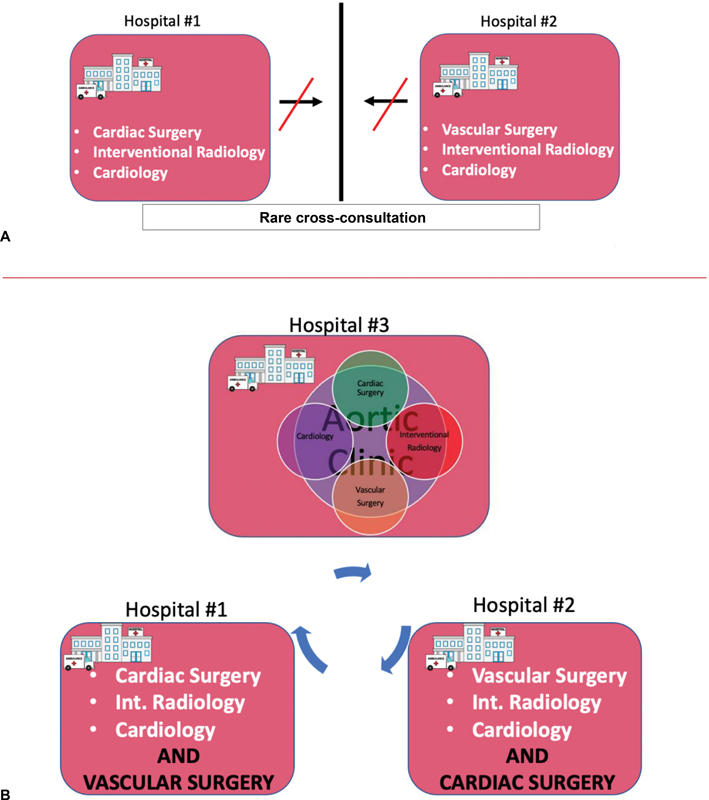
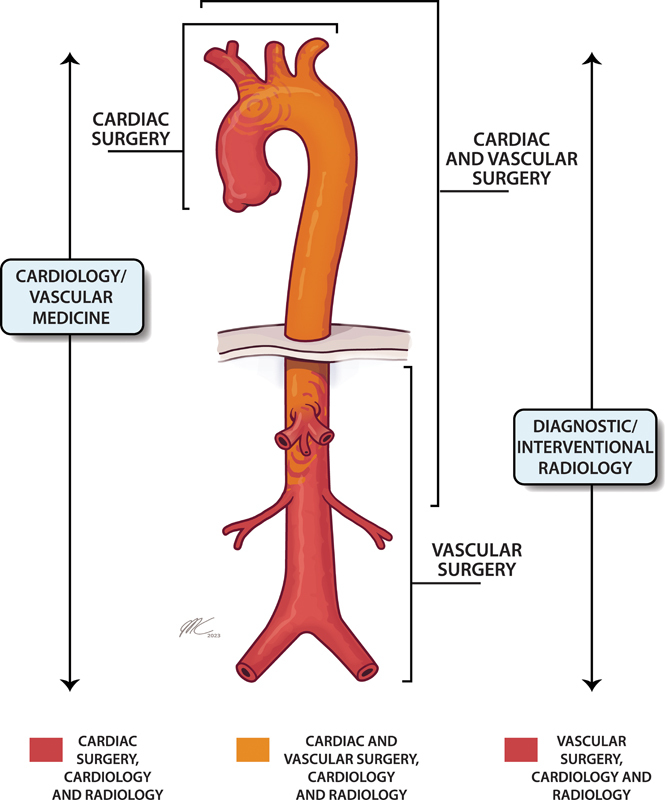
Methods: An Aortic Team care pathway was implemented in November 2019. Working as a unit, two cardiac surgeons, two vascular surgeons, an interventional radiologist, a cardiologist, and an anesthesiologist collectively determined care decisions via multispecialty presence at an Aortic Clinic. Cardiac and vascular surgeons operated in tandem for open procedures. Interventional radiology participated alongside cardiac and vascular for endovascular procedures. Cardiology aided in medical therapies for heritable and degenerative disease, and had a lead role for genetics and high-risk pregnancy referrals. The model spanned three hospitals. Clinical outcomes at 3 years were assessed.
Results: There were 35 descending thoracic and thoracoabdominal surgeries and 77 thoracic endovascular aortic repairs. Endoarch devices were used in 7 cases (Gore Thoracic Branch Endoprosthesis, 4, Terumo RelayBranch, 3) and an endothoracoabdominal device in 4 cases (Cook Zenith t-branch). The Aortic Clinic acquired 456 patients, with yearly increases (54 patients [year 1], 181 patients [year 2], 221 patients [year 3]). For surgery, mortality was 8.6% (3/35), permanent paralysis 5.7% (2/35), stroke 8.6% (3/35), permanent dialysis 0%, and reinterventions 8.6% (3/35). For endovascular cases, mortality was 3.9% (3/77), permanent paralysis 3.9% (3/77), stroke 5.2% (4/77), permanent dialysis 1.3% (1/77), and reinterventions 16.9% (13/77).
Conclusion: An Aortic Team model is feasible and ensures all treatment options are considered. Conventional open thoracoabdominal procedures showed acceptable outcomes. Endoarch technology shows early promise.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
