Ryan J Mulholland, Francesco Manca, Giorgio Ciminata, Terry J Quinn, Robert Trotter, Kevin G Pollock, Steven Lister, Claudia Geue
{"title":"评估口服抗凝剂处方的不平等对心房颤动患者疗效的影响。","authors":"Ryan J Mulholland, Francesco Manca, Giorgio Ciminata, Terry J Quinn, Robert Trotter, Kevin G Pollock, Steven Lister, Claudia Geue","doi":"10.1093/ehjopen/oeae016","DOIUrl":null,"url":null,"abstract":"<p><strong>Aims: </strong>Whilst anti-coagulation is typically recommended for thromboprophylaxis in atrial fibrillation (AF), it is often never prescribed or prematurely discontinued. The aim of this study was to evaluate the effect of inequalities in anti-coagulant prescribing by assessing stroke/systemic embolism (SSE) and bleeding risk in people with AF who continue anti-coagulation compared with those who stop transiently, permanently, or never start.</p><p><strong>Methods and results: </strong>This retrospective cohort study utilized linked Scottish healthcare data to identify adults diagnosed with AF between January 2010 and April 2016, with a CHA<sub>2</sub>DS<sub>2</sub>-VASC score of ≥2. They were sub-categorized based on anti-coagulant exposure: never started, continuous, discontinuous, and cessation. Inverse probability of treatment weighting-adjusted Cox regression and competing risk regression was utilized to compare SSE and bleeding risks between cohorts during 5-year follow-up. Of an overall cohort of 47 427 people, 26 277 (55.41%) were never anti-coagulated, 7934 (16.72%) received continuous anti-coagulation, 9107 (19.2%) temporarily discontinued, and 4109 (8.66%) permanently discontinued. Lower socio-economic status, elevated frailty score, and age ≥ 75 were associated with a reduced likelihood of initiation and continuation of anti-coagulation. Stroke/systemic embolism risk was significantly greater in those with discontinuous anti-coagulation, compared with continuous [subhazard ratio (SHR): 2.65; 2.39-2.94]. In the context of a major bleeding event, there was no significant difference in bleeding risk between the cessation and continuous cohorts (SHR 0.94; 0.42-2.14).</p><p><strong>Conclusion: </strong>Our data suggest significant inequalities in anti-coagulation prescribing, with substantial opportunity to improve initiation and continuation. Decision-making should be patient-centred and must recognize that discontinuation or cessation is associated with considerable thromboembolic risk not offset by mitigated bleeding risk.</p>","PeriodicalId":93995,"journal":{"name":"European heart journal open","volume":"4 2","pages":"oeae016"},"PeriodicalIF":0.0000,"publicationDate":"2024-03-05","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10989660/pdf/","citationCount":"0","resultStr":"{\"title\":\"Evaluating the effect of inequalities in oral anti-coagulant prescribing on outcomes in people with atrial fibrillation.\",\"authors\":\"Ryan J Mulholland, Francesco Manca, Giorgio Ciminata, Terry J Quinn, Robert Trotter, Kevin G Pollock, Steven Lister, Claudia Geue\",\"doi\":\"10.1093/ehjopen/oeae016\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Aims: </strong>Whilst anti-coagulation is typically recommended for thromboprophylaxis in atrial fibrillation (AF), it is often never prescribed or prematurely discontinued. The aim of this study was to evaluate the effect of inequalities in anti-coagulant prescribing by assessing stroke/systemic embolism (SSE) and bleeding risk in people with AF who continue anti-coagulation compared with those who stop transiently, permanently, or never start.</p><p><strong>Methods and results: </strong>This retrospective cohort study utilized linked Scottish healthcare data to identify adults diagnosed with AF between January 2010 and April 2016, with a CHA<sub>2</sub>DS<sub>2</sub>-VASC score of ≥2. They were sub-categorized based on anti-coagulant exposure: never started, continuous, discontinuous, and cessation. Inverse probability of treatment weighting-adjusted Cox regression and competing risk regression was utilized to compare SSE and bleeding risks between cohorts during 5-year follow-up. Of an overall cohort of 47 427 people, 26 277 (55.41%) were never anti-coagulated, 7934 (16.72%) received continuous anti-coagulation, 9107 (19.2%) temporarily discontinued, and 4109 (8.66%) permanently discontinued. Lower socio-economic status, elevated frailty score, and age ≥ 75 were associated with a reduced likelihood of initiation and continuation of anti-coagulation. Stroke/systemic embolism risk was significantly greater in those with discontinuous anti-coagulation, compared with continuous [subhazard ratio (SHR): 2.65; 2.39-2.94]. In the context of a major bleeding event, there was no significant difference in bleeding risk between the cessation and continuous cohorts (SHR 0.94; 0.42-2.14).</p><p><strong>Conclusion: </strong>Our data suggest significant inequalities in anti-coagulation prescribing, with substantial opportunity to improve initiation and continuation. Decision-making should be patient-centred and must recognize that discontinuation or cessation is associated with considerable thromboembolic risk not offset by mitigated bleeding risk.</p>\",\"PeriodicalId\":93995,\"journal\":{\"name\":\"European heart journal open\",\"volume\":\"4 2\",\"pages\":\"oeae016\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2024-03-05\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10989660/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"European heart journal open\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1093/ehjopen/oeae016\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2024/3/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"European heart journal open","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1093/ehjopen/oeae016","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/3/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
Evaluating the effect of inequalities in oral anti-coagulant prescribing on outcomes in people with atrial fibrillation.
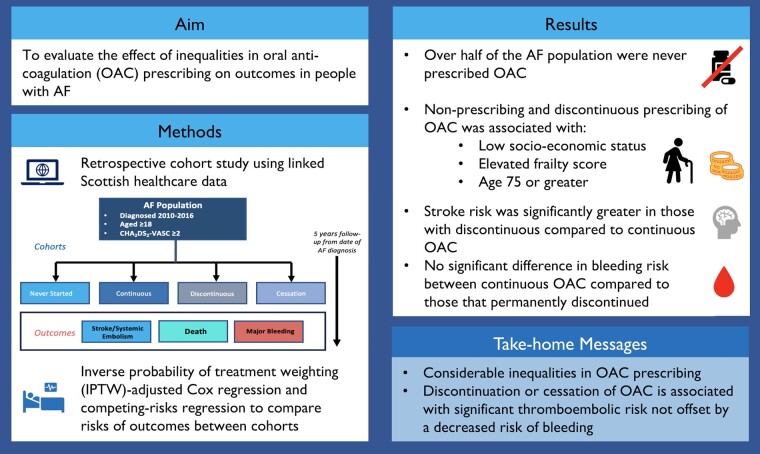
Aims: Whilst anti-coagulation is typically recommended for thromboprophylaxis in atrial fibrillation (AF), it is often never prescribed or prematurely discontinued. The aim of this study was to evaluate the effect of inequalities in anti-coagulant prescribing by assessing stroke/systemic embolism (SSE) and bleeding risk in people with AF who continue anti-coagulation compared with those who stop transiently, permanently, or never start.
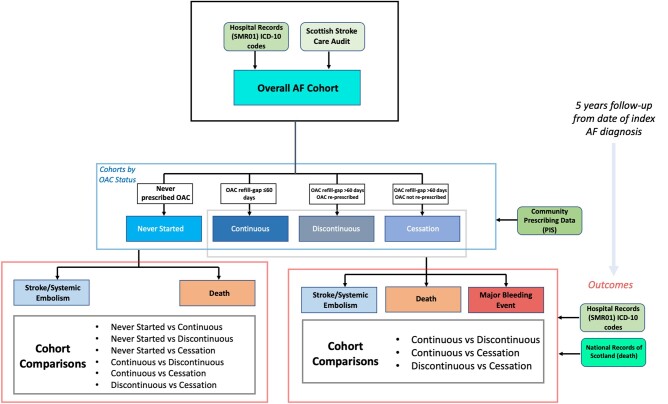
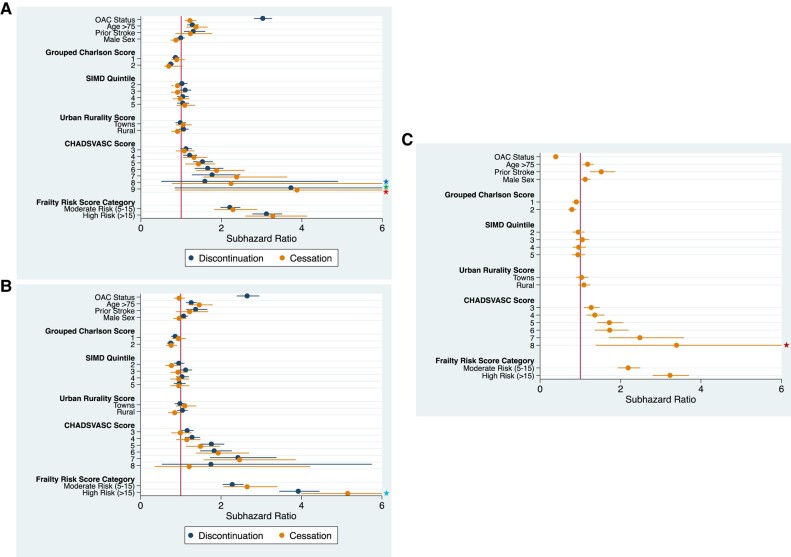
Methods and results: This retrospective cohort study utilized linked Scottish healthcare data to identify adults diagnosed with AF between January 2010 and April 2016, with a CHA2DS2-VASC score of ≥2. They were sub-categorized based on anti-coagulant exposure: never started, continuous, discontinuous, and cessation. Inverse probability of treatment weighting-adjusted Cox regression and competing risk regression was utilized to compare SSE and bleeding risks between cohorts during 5-year follow-up. Of an overall cohort of 47 427 people, 26 277 (55.41%) were never anti-coagulated, 7934 (16.72%) received continuous anti-coagulation, 9107 (19.2%) temporarily discontinued, and 4109 (8.66%) permanently discontinued. Lower socio-economic status, elevated frailty score, and age ≥ 75 were associated with a reduced likelihood of initiation and continuation of anti-coagulation. Stroke/systemic embolism risk was significantly greater in those with discontinuous anti-coagulation, compared with continuous [subhazard ratio (SHR): 2.65; 2.39-2.94]. In the context of a major bleeding event, there was no significant difference in bleeding risk between the cessation and continuous cohorts (SHR 0.94; 0.42-2.14).
Conclusion: Our data suggest significant inequalities in anti-coagulation prescribing, with substantial opportunity to improve initiation and continuation. Decision-making should be patient-centred and must recognize that discontinuation or cessation is associated with considerable thromboembolic risk not offset by mitigated bleeding risk.


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
