Sophie Cole, Sian Noble, Rachael Gooberman-Hill, Rafael Pinedo-Villanueva
{"title":"针对全膝关节置换术后慢性疼痛的支持与治疗(STAR)护理路径与常规护理的成本效益模型分析。","authors":"Sophie Cole, Sian Noble, Rachael Gooberman-Hill, Rafael Pinedo-Villanueva","doi":"10.1186/s12962-024-00532-5","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>The aim of the study was to estimate the long-term cost-effectiveness of the Support and Treatment After Replacement (STAR) care pathway for chronic pain after total knee replacement compared with usual postoperative care.</p><p><strong>Methods: </strong>Study design: A decision-analytic (cohort Markov) model was used for the simulation with time dependent annual transition probabilities and a time horizon of five years.</p><p><strong>Setting: </strong>Patients treated by National Health Service (NHS) hospitals in England and Wales.</p><p><strong>Study population: </strong>Adults classified as having chronic pain three months after undergoing a total knee replacement.</p><p><strong>Intervention: </strong>The STAR care pathway following a total knee replacement.</p><p><strong>Comparator: </strong>Usual postoperative care following a total knee replacement.</p><p><strong>Perspective: </strong>The study was undertaken from the perspective of the NHS.</p><p><strong>Outcome measures: </strong>Quality-adjusted life years and healthcare costs. Discounting: A rate of 3.5% for both costs and health utility.</p><p><strong>Results: </strong>Model results indicate that the STAR intervention would dominate current practice by providing a gain in quality-adjusted life years (QALYs) of 0.086 and a reduction of £375 (per person) in costs over the first five years. The incremental net monetary benefit of the STAR intervention was estimated at £2,086 (at a threshold of £20,000 per QALY). Probabilistic sensitivity analysis suggests the STAR intervention is likely to be cost-effective with a probability of 0.62. The results remain robust to changes in model assumptions on comparator utility and the timing of the start of the intervention. If hospital admission costs are assumed not to be reduced by the STAR intervention, it would no longer be cost saving, but it would likely be cost-effective based on probabilistic sensitivity analysis (0.59).</p><p><strong>Conclusion: </strong>Evidence from the economic model suggests that the STAR care pathway is likely to be cost-effective and potentially dominant from an NHS perspective.</p><p><strong>Trial registration: </strong>The STAR trial is registered with ISRCTN, ISRCTN92545361.</p>","PeriodicalId":47054,"journal":{"name":"Cost Effectiveness and Resource Allocation","volume":"22 1","pages":"28"},"PeriodicalIF":2.5000,"publicationDate":"2024-04-11","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11010279/pdf/","citationCount":"0","resultStr":"{\"title\":\"Modelled cost-effectiveness analysis of the Support and Treatment After Replacement (STAR) care pathway for chronic pain after total knee replacement compared with usual care.\",\"authors\":\"Sophie Cole, Sian Noble, Rachael Gooberman-Hill, Rafael Pinedo-Villanueva\",\"doi\":\"10.1186/s12962-024-00532-5\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>The aim of the study was to estimate the long-term cost-effectiveness of the Support and Treatment After Replacement (STAR) care pathway for chronic pain after total knee replacement compared with usual postoperative care.</p><p><strong>Methods: </strong>Study design: A decision-analytic (cohort Markov) model was used for the simulation with time dependent annual transition probabilities and a time horizon of five years.</p><p><strong>Setting: </strong>Patients treated by National Health Service (NHS) hospitals in England and Wales.</p><p><strong>Study population: </strong>Adults classified as having chronic pain three months after undergoing a total knee replacement.</p><p><strong>Intervention: </strong>The STAR care pathway following a total knee replacement.</p><p><strong>Comparator: </strong>Usual postoperative care following a total knee replacement.</p><p><strong>Perspective: </strong>The study was undertaken from the perspective of the NHS.</p><p><strong>Outcome measures: </strong>Quality-adjusted life years and healthcare costs. Discounting: A rate of 3.5% for both costs and health utility.</p><p><strong>Results: </strong>Model results indicate that the STAR intervention would dominate current practice by providing a gain in quality-adjusted life years (QALYs) of 0.086 and a reduction of £375 (per person) in costs over the first five years. The incremental net monetary benefit of the STAR intervention was estimated at £2,086 (at a threshold of £20,000 per QALY). Probabilistic sensitivity analysis suggests the STAR intervention is likely to be cost-effective with a probability of 0.62. The results remain robust to changes in model assumptions on comparator utility and the timing of the start of the intervention. If hospital admission costs are assumed not to be reduced by the STAR intervention, it would no longer be cost saving, but it would likely be cost-effective based on probabilistic sensitivity analysis (0.59).</p><p><strong>Conclusion: </strong>Evidence from the economic model suggests that the STAR care pathway is likely to be cost-effective and potentially dominant from an NHS perspective.</p><p><strong>Trial registration: </strong>The STAR trial is registered with ISRCTN, ISRCTN92545361.</p>\",\"PeriodicalId\":47054,\"journal\":{\"name\":\"Cost Effectiveness and Resource Allocation\",\"volume\":\"22 1\",\"pages\":\"28\"},\"PeriodicalIF\":2.5000,\"publicationDate\":\"2024-04-11\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11010279/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Cost Effectiveness and Resource Allocation\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1186/s12962-024-00532-5\",\"RegionNum\":4,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q3\",\"JCRName\":\"HEALTH POLICY & SERVICES\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Cost Effectiveness and Resource Allocation","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1186/s12962-024-00532-5","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"HEALTH POLICY & SERVICES","Score":null,"Total":0}
Modelled cost-effectiveness analysis of the Support and Treatment After Replacement (STAR) care pathway for chronic pain after total knee replacement compared with usual care.
Background: The aim of the study was to estimate the long-term cost-effectiveness of the Support and Treatment After Replacement (STAR) care pathway for chronic pain after total knee replacement compared with usual postoperative care.
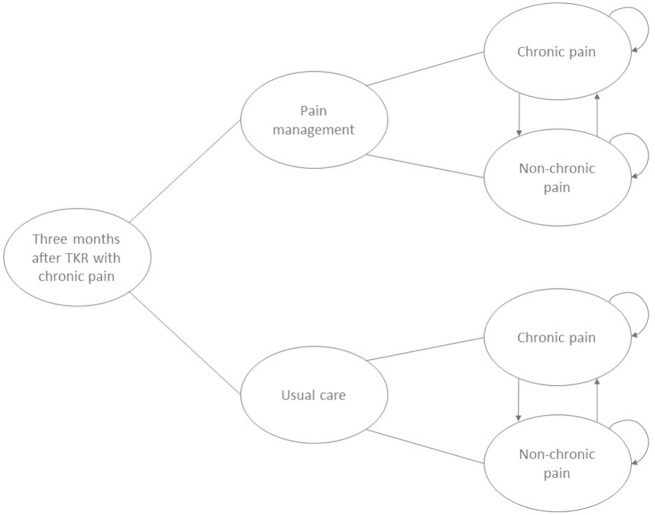
Methods: Study design: A decision-analytic (cohort Markov) model was used for the simulation with time dependent annual transition probabilities and a time horizon of five years.
Setting: Patients treated by National Health Service (NHS) hospitals in England and Wales.
Study population: Adults classified as having chronic pain three months after undergoing a total knee replacement.
Intervention: The STAR care pathway following a total knee replacement.
Comparator: Usual postoperative care following a total knee replacement.
Perspective: The study was undertaken from the perspective of the NHS.
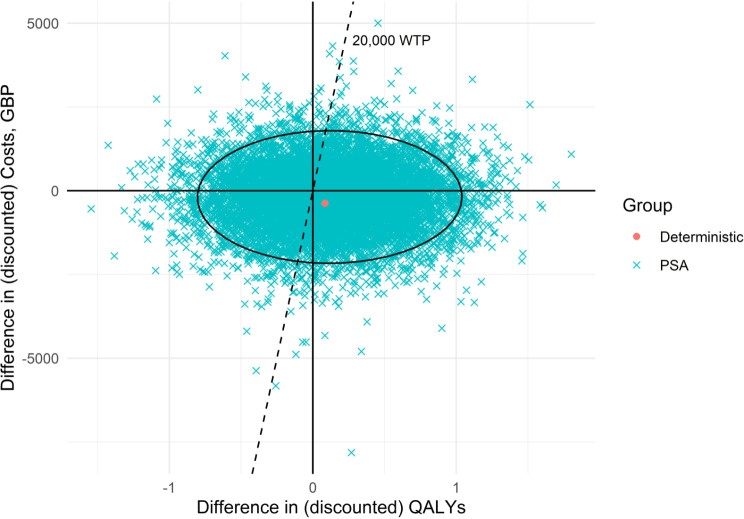
Outcome measures: Quality-adjusted life years and healthcare costs. Discounting: A rate of 3.5% for both costs and health utility.
Results: Model results indicate that the STAR intervention would dominate current practice by providing a gain in quality-adjusted life years (QALYs) of 0.086 and a reduction of £375 (per person) in costs over the first five years. The incremental net monetary benefit of the STAR intervention was estimated at £2,086 (at a threshold of £20,000 per QALY). Probabilistic sensitivity analysis suggests the STAR intervention is likely to be cost-effective with a probability of 0.62. The results remain robust to changes in model assumptions on comparator utility and the timing of the start of the intervention. If hospital admission costs are assumed not to be reduced by the STAR intervention, it would no longer be cost saving, but it would likely be cost-effective based on probabilistic sensitivity analysis (0.59).
Conclusion: Evidence from the economic model suggests that the STAR care pathway is likely to be cost-effective and potentially dominant from an NHS perspective.
Trial registration: The STAR trial is registered with ISRCTN, ISRCTN92545361.
期刊介绍:
Cost Effectiveness and Resource Allocation is an Open Access, peer-reviewed, online journal that considers manuscripts on all aspects of cost-effectiveness analysis, including conceptual or methodological work, economic evaluations, and policy analysis related to resource allocation at a national or international level. Cost Effectiveness and Resource Allocation is aimed at health economists, health services researchers, and policy-makers with an interest in enhancing the flow and transfer of knowledge relating to efficiency in the health sector. Manuscripts are encouraged from researchers based in low- and middle-income countries, with a view to increasing the international economic evidence base for health.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
