{"title":"老龄人口的高血压和虚弱双重负担:降低血压能改善预后吗?","authors":"Meiling Piao MD, Vipin Kumar MD, Chunzi Jin MD, PhD, Xian Wu Cheng MD, PhD, FAHA","doi":"10.1111/jch.14830","DOIUrl":null,"url":null,"abstract":"<p>Frailty, a geriatric syndrome characterized by multiple declining physiological reserves, reduced resistance to stressors, increased vulnerability, and impaired homeostatic maintenance is associated with increased risks of disability, hospitalization, and mortality in older adults.<span><sup>1</sup></span> The recognition of frailty as a health concern has led to increased research regarding the relationship between frailty and hypertension, and emerging evidence suggests a reciprocal relationship between frailty and hypertension in older adults. Chronic conditions such as hypertension are significant contributors to frailty, and cardiovascular complications resulting from hypertension have been identified as factors that contribute to the onset of frailty.<span><sup>2</sup></span> Conversely, frailty has been suggested to be a risk factor for cardiovascular disease including hypertension.<span><sup>3</sup></span> The management of hypertension in frail older adults requires a comprehensive, multidimensional approach that focuses on improving overall health, effective blood pressure control, and physical function. However, the management of hypertension in frail older adults remains a challenge as several investigations have indicated that while treatment may provide cardiovascular benefits, antihypertensive medications may also increase the risk of adverse events such as hypotension, falls, and related injuries.<span><sup>4, 5</sup></span></p><p>An evolving concept in the management of hypertension in frail older adults is the “Blood Pressure Time in Target Range (BP-TTR),” which indicates the percentage of time that an individual's BP remains within a predefined target range (Figure 1). The post hoc analysis of the Systolic Blood Pressure Intervention Trial (SPRINT) by Zhu et al. provides valuable insights into the relationship between maintaining BP-TTR and reducing cardiovascular risks in patients with both hypertension and prefrailty or frailty.<span><sup>6</sup></span> The Zhu et al. study highlights the critical importance of monitoring and controlling both the systolic blood pressure (SBP)-TTR and the diastolic blood pressure (DBP)-TTR to reduce cardiovascular risks, and they obtained four important findings: (<i>i</i>) The maintenance of SBP in the target range is crucial, as lower SBP-TTR values were correlated with an increased incidence of the study's primary outcome, that is, cardiovascular events; (<i>ii</i>) higher SBP-TTR values were associated with a reduced risk of cardiovascular outcomes, highlighting the protective effect of maintaining SBP within a higher target range; (<i>iii</i>) similar patterns were observed for the DBP-TTR, suggesting that the careful management of both SBP and DBP is critical in this patient population; and (<i>iv</i>) a subgroup analysis suggested that the protective effect of higher SBP-TTR values was less pronounced at lower DBP-TTR values, highlighting the interplay between SBP and DBP management.</p><p>Another of the key findings of the study by Zhu and colleagues was a notable association between elevated SBP-TTR and a reduced risk of primary outcomes independent of intensive blood pressure management. Their findings have important clinical implications, that is, that even when patients are undergoing intensive antihypertensive therapy to maintain their SBP below 120 mmHg, their prognoses may be improved by emphasizing the SBP-TTR and implementing interventions to prolong the SBP-TTR, which is consistent with earlier findings.<span><sup>7</sup></span> However, a retrospective analysis of the SPRINT data showed that frail individuals may benefit from intensive blood pressure control without an increased risk of serious adverse events.<span><sup>8</sup></span> It is therefore essential to identify appropriate metrics to assess the effectiveness of blood pressure control in patients with hypertension and high cardiovascular risk, as doing so will optimize pharmacological treatment approaches and inform future clinical trials aimed at improving prognostic outcomes.</p><p>In the Zhu et al. study, the patients' DBP-TTR values were similar to their SBP-TTR levels. After adjustment by a multivariate Cox regression analysis, neither the SBP-TTR nor the DBP-TTR showed a significant association with safety outcomes. A subgroup analysis revealed a significant interaction between the SBP-TTR and the DBP-TTR, suggesting that the effect of the SBP-TTR on the primary outcome was attenuated in cases of low DBP-TTR values. It is important to note that the Zhu et al. findings underscore the possibility that the impact of the SBP-TTR on the primary outcome was less pronounced in cases with lower DBP-TTR values. Moreover, the authors categorized the DBP-TTR levels into two groups to investigate the possibility that the observed interaction between high DBP-TTR group and low DBP-TTR group may be due to underlying differences in the patients' baseline characteristics.</p><p>Despite its insightful findings, the Zhu et al. study acknowledges its limitations — such as the exclusion of extremely frail individuals from the SPRINT — which may limit the generalizability of their conclusions to the broader frail population. In addition, as a post hoc analysis, the study's findings may have been influenced by biases inherent in such a study design. Prospective research is necessary to further test the Zhu et al. findings and to investigate whether interventions aimed at increasing BP-TTR values could improve long-term outcomes in patients with low baseline BP-TTR levels.</p><p>In conclusion, the study reported by Zhu and colleagues in this issue of <i>The Journal of Clinical Hypertension</i> contributes significantly to the evolving understanding of hypertension management in frail and prefrail populations. Maintaining BP within a target range is necessary to mitigate cardiovascular risks in frail and prefrail elderly patients. The findings described above suggest the need for a more nuanced approach to hypertension management in clinical practice, taking into account the dynamic nature of BP and the unique needs of this vulnerable population. As the global population continues to age, it is increasingly important to understand and address the complex interplay among frailty, hypertension, and cardiovascular risks in promoting health and longevity.</p><p>Meiling Piao wrote the first draft of the manuscript. Vipin Kumar and Chunzi Jin edited the manuscript. Xian Wu Cheng handled the funding and supervision.</p><p>The authors declare no potential conflicts of interest with respect to the research, authorship, and/or publication of this manuscript.</p>","PeriodicalId":50237,"journal":{"name":"Journal of Clinical Hypertension","volume":"26 6","pages":"740-742"},"PeriodicalIF":2.5000,"publicationDate":"2024-05-07","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11180687/pdf/","citationCount":"0","resultStr":"{\"title\":\"The double burden of hypertension and frailty in the aging population: Does lowering blood pressure improve outcomes?\",\"authors\":\"Meiling Piao MD, Vipin Kumar MD, Chunzi Jin MD, PhD, Xian Wu Cheng MD, PhD, FAHA\",\"doi\":\"10.1111/jch.14830\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p>Frailty, a geriatric syndrome characterized by multiple declining physiological reserves, reduced resistance to stressors, increased vulnerability, and impaired homeostatic maintenance is associated with increased risks of disability, hospitalization, and mortality in older adults.<span><sup>1</sup></span> The recognition of frailty as a health concern has led to increased research regarding the relationship between frailty and hypertension, and emerging evidence suggests a reciprocal relationship between frailty and hypertension in older adults. Chronic conditions such as hypertension are significant contributors to frailty, and cardiovascular complications resulting from hypertension have been identified as factors that contribute to the onset of frailty.<span><sup>2</sup></span> Conversely, frailty has been suggested to be a risk factor for cardiovascular disease including hypertension.<span><sup>3</sup></span> The management of hypertension in frail older adults requires a comprehensive, multidimensional approach that focuses on improving overall health, effective blood pressure control, and physical function. However, the management of hypertension in frail older adults remains a challenge as several investigations have indicated that while treatment may provide cardiovascular benefits, antihypertensive medications may also increase the risk of adverse events such as hypotension, falls, and related injuries.<span><sup>4, 5</sup></span></p><p>An evolving concept in the management of hypertension in frail older adults is the “Blood Pressure Time in Target Range (BP-TTR),” which indicates the percentage of time that an individual's BP remains within a predefined target range (Figure 1). The post hoc analysis of the Systolic Blood Pressure Intervention Trial (SPRINT) by Zhu et al. provides valuable insights into the relationship between maintaining BP-TTR and reducing cardiovascular risks in patients with both hypertension and prefrailty or frailty.<span><sup>6</sup></span> The Zhu et al. study highlights the critical importance of monitoring and controlling both the systolic blood pressure (SBP)-TTR and the diastolic blood pressure (DBP)-TTR to reduce cardiovascular risks, and they obtained four important findings: (<i>i</i>) The maintenance of SBP in the target range is crucial, as lower SBP-TTR values were correlated with an increased incidence of the study's primary outcome, that is, cardiovascular events; (<i>ii</i>) higher SBP-TTR values were associated with a reduced risk of cardiovascular outcomes, highlighting the protective effect of maintaining SBP within a higher target range; (<i>iii</i>) similar patterns were observed for the DBP-TTR, suggesting that the careful management of both SBP and DBP is critical in this patient population; and (<i>iv</i>) a subgroup analysis suggested that the protective effect of higher SBP-TTR values was less pronounced at lower DBP-TTR values, highlighting the interplay between SBP and DBP management.</p><p>Another of the key findings of the study by Zhu and colleagues was a notable association between elevated SBP-TTR and a reduced risk of primary outcomes independent of intensive blood pressure management. Their findings have important clinical implications, that is, that even when patients are undergoing intensive antihypertensive therapy to maintain their SBP below 120 mmHg, their prognoses may be improved by emphasizing the SBP-TTR and implementing interventions to prolong the SBP-TTR, which is consistent with earlier findings.<span><sup>7</sup></span> However, a retrospective analysis of the SPRINT data showed that frail individuals may benefit from intensive blood pressure control without an increased risk of serious adverse events.<span><sup>8</sup></span> It is therefore essential to identify appropriate metrics to assess the effectiveness of blood pressure control in patients with hypertension and high cardiovascular risk, as doing so will optimize pharmacological treatment approaches and inform future clinical trials aimed at improving prognostic outcomes.</p><p>In the Zhu et al. study, the patients' DBP-TTR values were similar to their SBP-TTR levels. After adjustment by a multivariate Cox regression analysis, neither the SBP-TTR nor the DBP-TTR showed a significant association with safety outcomes. A subgroup analysis revealed a significant interaction between the SBP-TTR and the DBP-TTR, suggesting that the effect of the SBP-TTR on the primary outcome was attenuated in cases of low DBP-TTR values. It is important to note that the Zhu et al. findings underscore the possibility that the impact of the SBP-TTR on the primary outcome was less pronounced in cases with lower DBP-TTR values. Moreover, the authors categorized the DBP-TTR levels into two groups to investigate the possibility that the observed interaction between high DBP-TTR group and low DBP-TTR group may be due to underlying differences in the patients' baseline characteristics.</p><p>Despite its insightful findings, the Zhu et al. study acknowledges its limitations — such as the exclusion of extremely frail individuals from the SPRINT — which may limit the generalizability of their conclusions to the broader frail population. In addition, as a post hoc analysis, the study's findings may have been influenced by biases inherent in such a study design. Prospective research is necessary to further test the Zhu et al. findings and to investigate whether interventions aimed at increasing BP-TTR values could improve long-term outcomes in patients with low baseline BP-TTR levels.</p><p>In conclusion, the study reported by Zhu and colleagues in this issue of <i>The Journal of Clinical Hypertension</i> contributes significantly to the evolving understanding of hypertension management in frail and prefrail populations. Maintaining BP within a target range is necessary to mitigate cardiovascular risks in frail and prefrail elderly patients. The findings described above suggest the need for a more nuanced approach to hypertension management in clinical practice, taking into account the dynamic nature of BP and the unique needs of this vulnerable population. As the global population continues to age, it is increasingly important to understand and address the complex interplay among frailty, hypertension, and cardiovascular risks in promoting health and longevity.</p><p>Meiling Piao wrote the first draft of the manuscript. Vipin Kumar and Chunzi Jin edited the manuscript. Xian Wu Cheng handled the funding and supervision.</p><p>The authors declare no potential conflicts of interest with respect to the research, authorship, and/or publication of this manuscript.</p>\",\"PeriodicalId\":50237,\"journal\":{\"name\":\"Journal of Clinical Hypertension\",\"volume\":\"26 6\",\"pages\":\"740-742\"},\"PeriodicalIF\":2.5000,\"publicationDate\":\"2024-05-07\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11180687/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of Clinical Hypertension\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://onlinelibrary.wiley.com/doi/10.1111/jch.14830\",\"RegionNum\":3,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q2\",\"JCRName\":\"PERIPHERAL VASCULAR DISEASE\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Clinical Hypertension","FirstCategoryId":"3","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1111/jch.14830","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"PERIPHERAL VASCULAR DISEASE","Score":null,"Total":0}
The double burden of hypertension and frailty in the aging population: Does lowering blood pressure improve outcomes?
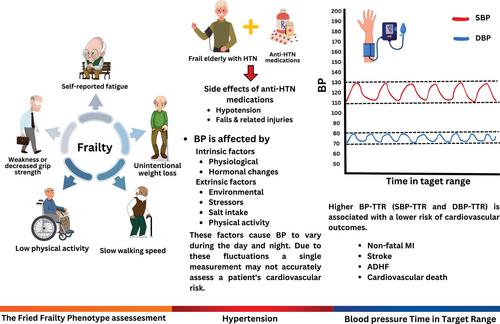
Frailty, a geriatric syndrome characterized by multiple declining physiological reserves, reduced resistance to stressors, increased vulnerability, and impaired homeostatic maintenance is associated with increased risks of disability, hospitalization, and mortality in older adults.1 The recognition of frailty as a health concern has led to increased research regarding the relationship between frailty and hypertension, and emerging evidence suggests a reciprocal relationship between frailty and hypertension in older adults. Chronic conditions such as hypertension are significant contributors to frailty, and cardiovascular complications resulting from hypertension have been identified as factors that contribute to the onset of frailty.2 Conversely, frailty has been suggested to be a risk factor for cardiovascular disease including hypertension.3 The management of hypertension in frail older adults requires a comprehensive, multidimensional approach that focuses on improving overall health, effective blood pressure control, and physical function. However, the management of hypertension in frail older adults remains a challenge as several investigations have indicated that while treatment may provide cardiovascular benefits, antihypertensive medications may also increase the risk of adverse events such as hypotension, falls, and related injuries.4, 5
An evolving concept in the management of hypertension in frail older adults is the “Blood Pressure Time in Target Range (BP-TTR),” which indicates the percentage of time that an individual's BP remains within a predefined target range (Figure 1). The post hoc analysis of the Systolic Blood Pressure Intervention Trial (SPRINT) by Zhu et al. provides valuable insights into the relationship between maintaining BP-TTR and reducing cardiovascular risks in patients with both hypertension and prefrailty or frailty.6 The Zhu et al. study highlights the critical importance of monitoring and controlling both the systolic blood pressure (SBP)-TTR and the diastolic blood pressure (DBP)-TTR to reduce cardiovascular risks, and they obtained four important findings: (i) The maintenance of SBP in the target range is crucial, as lower SBP-TTR values were correlated with an increased incidence of the study's primary outcome, that is, cardiovascular events; (ii) higher SBP-TTR values were associated with a reduced risk of cardiovascular outcomes, highlighting the protective effect of maintaining SBP within a higher target range; (iii) similar patterns were observed for the DBP-TTR, suggesting that the careful management of both SBP and DBP is critical in this patient population; and (iv) a subgroup analysis suggested that the protective effect of higher SBP-TTR values was less pronounced at lower DBP-TTR values, highlighting the interplay between SBP and DBP management.
Another of the key findings of the study by Zhu and colleagues was a notable association between elevated SBP-TTR and a reduced risk of primary outcomes independent of intensive blood pressure management. Their findings have important clinical implications, that is, that even when patients are undergoing intensive antihypertensive therapy to maintain their SBP below 120 mmHg, their prognoses may be improved by emphasizing the SBP-TTR and implementing interventions to prolong the SBP-TTR, which is consistent with earlier findings.7 However, a retrospective analysis of the SPRINT data showed that frail individuals may benefit from intensive blood pressure control without an increased risk of serious adverse events.8 It is therefore essential to identify appropriate metrics to assess the effectiveness of blood pressure control in patients with hypertension and high cardiovascular risk, as doing so will optimize pharmacological treatment approaches and inform future clinical trials aimed at improving prognostic outcomes.
In the Zhu et al. study, the patients' DBP-TTR values were similar to their SBP-TTR levels. After adjustment by a multivariate Cox regression analysis, neither the SBP-TTR nor the DBP-TTR showed a significant association with safety outcomes. A subgroup analysis revealed a significant interaction between the SBP-TTR and the DBP-TTR, suggesting that the effect of the SBP-TTR on the primary outcome was attenuated in cases of low DBP-TTR values. It is important to note that the Zhu et al. findings underscore the possibility that the impact of the SBP-TTR on the primary outcome was less pronounced in cases with lower DBP-TTR values. Moreover, the authors categorized the DBP-TTR levels into two groups to investigate the possibility that the observed interaction between high DBP-TTR group and low DBP-TTR group may be due to underlying differences in the patients' baseline characteristics.
Despite its insightful findings, the Zhu et al. study acknowledges its limitations — such as the exclusion of extremely frail individuals from the SPRINT — which may limit the generalizability of their conclusions to the broader frail population. In addition, as a post hoc analysis, the study's findings may have been influenced by biases inherent in such a study design. Prospective research is necessary to further test the Zhu et al. findings and to investigate whether interventions aimed at increasing BP-TTR values could improve long-term outcomes in patients with low baseline BP-TTR levels.
In conclusion, the study reported by Zhu and colleagues in this issue of The Journal of Clinical Hypertension contributes significantly to the evolving understanding of hypertension management in frail and prefrail populations. Maintaining BP within a target range is necessary to mitigate cardiovascular risks in frail and prefrail elderly patients. The findings described above suggest the need for a more nuanced approach to hypertension management in clinical practice, taking into account the dynamic nature of BP and the unique needs of this vulnerable population. As the global population continues to age, it is increasingly important to understand and address the complex interplay among frailty, hypertension, and cardiovascular risks in promoting health and longevity.
Meiling Piao wrote the first draft of the manuscript. Vipin Kumar and Chunzi Jin edited the manuscript. Xian Wu Cheng handled the funding and supervision.
The authors declare no potential conflicts of interest with respect to the research, authorship, and/or publication of this manuscript.
期刊介绍:
The Journal of Clinical Hypertension is a peer-reviewed, monthly publication that serves internists, cardiologists, nephrologists, endocrinologists, hypertension specialists, primary care practitioners, pharmacists and all professionals interested in hypertension by providing objective, up-to-date information and practical recommendations on the full range of clinical aspects of hypertension. Commentaries and columns by experts in the field provide further insights into our original research articles as well as on major articles published elsewhere. Major guidelines for the management of hypertension are also an important feature of the Journal. Through its partnership with the World Hypertension League, JCH will include a new focus on hypertension and public health, including major policy issues, that features research and reviews related to disease characteristics and management at the population level.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
