Michael Brendan Cloney, Pavlos Texakalidis, Anastasios G Roumeliotis, Vineeth Thirunavu, Nathan A Shlobin, Kevin Swong, Najib El Tecle, Nader S Dahdaleh
{"title":"有寰椎骨折和无寰椎骨折的外伤性颅骨骨折患者在人口统计学、临床和管理方面的差异。","authors":"Michael Brendan Cloney, Pavlos Texakalidis, Anastasios G Roumeliotis, Vineeth Thirunavu, Nathan A Shlobin, Kevin Swong, Najib El Tecle, Nader S Dahdaleh","doi":"10.4103/jcvjs.jcvjs_147_23","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>Atlas fractures often accompany traumatic dens fractures, but existing literature on the management of simultaneous atlantoaxial fractures is limited.</p><p><strong>Methods: </strong>We examined all patients with traumatic dens fractures at our institution between 2008 and 2018. We used multivariable logistic regression and ordinal logistic regression to identify factors independently associated with presentation with a simultaneous atlas fracture, as well myelopathy severity, fracture nonunion, and selection for surgery.</p><p><strong>Results: </strong>Two hundred and eighty-two patients with traumatic dens fractures without subaxial fractures were identified, including 65 (22.8%) with simultaneous atlas fractures. The distribution of injury mechanisms differed between groups (χ<sup>2</sup> <i>P</i> = 0.0360). On multivariable logistic regression, dens nonunion was positively associated with type II fractures (odds ratio [OR] = 2.00, <i>P</i> = 0.038) and negatively associated with having surgery (OR = 0.52, <i>P</i> = 0.049), but not with having a C1 fracture (<i>P</i> = 0.3673). Worse myelopathy severity on presentation was associated with having a severe injury severity score (OR = 102.3, <i>P</i> < 0.001) and older age (OR = 1.28, <i>P</i> = 0.002), but not with having an atlas fracture (<i>P</i> = 0.2446). Having a simultaneous atlas fracture was associated with older age (OR = 1.29, <i>P</i> = 0.024) and dens fracture angulation (OR = 2.62, <i>P</i> = 0.004). Among patients who underwent surgery, C1/C2 posterior fusion was the most common procedure, and having a simultaneous atlas fracture was associated with selection for occipitocervical fusion (OCF) (OR = 14.35, <i>P</i> = 0.010).</p><p><strong>Conclusions: </strong>Among patients with traumatic dens, patients who have simultaneous atlas fractures are a distinct subpopulation with respect to age, mechanism of injury, fracture morphology, and management. Traumatic dens fractures with simultaneous atlas fractures are independently associated with selection for OCF rather than posterior cervical fusion alone.</p>","PeriodicalId":51721,"journal":{"name":"Journal of Craniovertebral Junction and Spine","volume":"15 1","pages":"21-29"},"PeriodicalIF":1.3000,"publicationDate":"2024-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11029115/pdf/","citationCount":"0","resultStr":"{\"title\":\"The demographic, clinical, and management differences between traumatic dens fracture patients with and without simultaneous atlas fractures.\",\"authors\":\"Michael Brendan Cloney, Pavlos Texakalidis, Anastasios G Roumeliotis, Vineeth Thirunavu, Nathan A Shlobin, Kevin Swong, Najib El Tecle, Nader S Dahdaleh\",\"doi\":\"10.4103/jcvjs.jcvjs_147_23\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Introduction: </strong>Atlas fractures often accompany traumatic dens fractures, but existing literature on the management of simultaneous atlantoaxial fractures is limited.</p><p><strong>Methods: </strong>We examined all patients with traumatic dens fractures at our institution between 2008 and 2018. We used multivariable logistic regression and ordinal logistic regression to identify factors independently associated with presentation with a simultaneous atlas fracture, as well myelopathy severity, fracture nonunion, and selection for surgery.</p><p><strong>Results: </strong>Two hundred and eighty-two patients with traumatic dens fractures without subaxial fractures were identified, including 65 (22.8%) with simultaneous atlas fractures. The distribution of injury mechanisms differed between groups (χ<sup>2</sup> <i>P</i> = 0.0360). On multivariable logistic regression, dens nonunion was positively associated with type II fractures (odds ratio [OR] = 2.00, <i>P</i> = 0.038) and negatively associated with having surgery (OR = 0.52, <i>P</i> = 0.049), but not with having a C1 fracture (<i>P</i> = 0.3673). Worse myelopathy severity on presentation was associated with having a severe injury severity score (OR = 102.3, <i>P</i> < 0.001) and older age (OR = 1.28, <i>P</i> = 0.002), but not with having an atlas fracture (<i>P</i> = 0.2446). Having a simultaneous atlas fracture was associated with older age (OR = 1.29, <i>P</i> = 0.024) and dens fracture angulation (OR = 2.62, <i>P</i> = 0.004). Among patients who underwent surgery, C1/C2 posterior fusion was the most common procedure, and having a simultaneous atlas fracture was associated with selection for occipitocervical fusion (OCF) (OR = 14.35, <i>P</i> = 0.010).</p><p><strong>Conclusions: </strong>Among patients with traumatic dens, patients who have simultaneous atlas fractures are a distinct subpopulation with respect to age, mechanism of injury, fracture morphology, and management. Traumatic dens fractures with simultaneous atlas fractures are independently associated with selection for OCF rather than posterior cervical fusion alone.</p>\",\"PeriodicalId\":51721,\"journal\":{\"name\":\"Journal of Craniovertebral Junction and Spine\",\"volume\":\"15 1\",\"pages\":\"21-29\"},\"PeriodicalIF\":1.3000,\"publicationDate\":\"2024-01-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11029115/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of Craniovertebral Junction and Spine\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.4103/jcvjs.jcvjs_147_23\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2024/3/13 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q2\",\"JCRName\":\"OTORHINOLARYNGOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Craniovertebral Junction and Spine","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.4103/jcvjs.jcvjs_147_23","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/3/13 0:00:00","PubModel":"Epub","JCR":"Q2","JCRName":"OTORHINOLARYNGOLOGY","Score":null,"Total":0}
The demographic, clinical, and management differences between traumatic dens fracture patients with and without simultaneous atlas fractures.
Introduction: Atlas fractures often accompany traumatic dens fractures, but existing literature on the management of simultaneous atlantoaxial fractures is limited.
Methods: We examined all patients with traumatic dens fractures at our institution between 2008 and 2018. We used multivariable logistic regression and ordinal logistic regression to identify factors independently associated with presentation with a simultaneous atlas fracture, as well myelopathy severity, fracture nonunion, and selection for surgery.
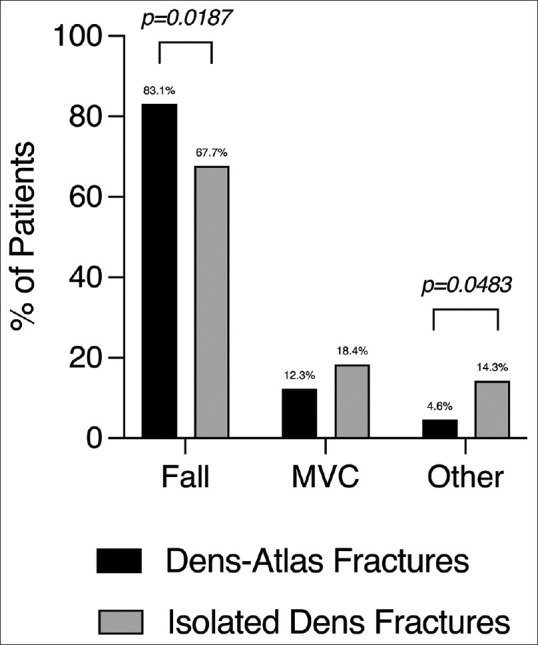
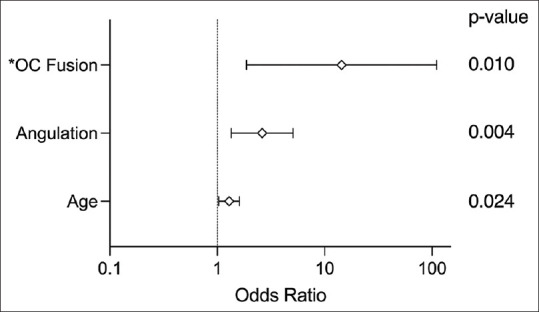
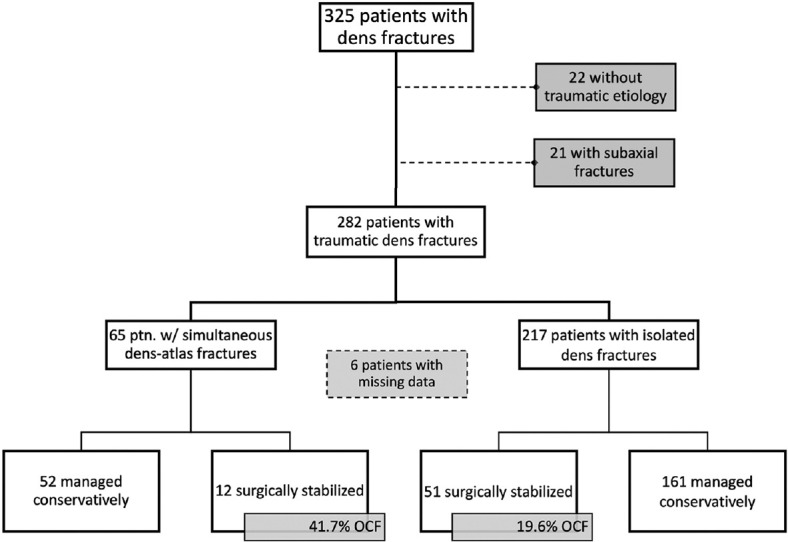
Results: Two hundred and eighty-two patients with traumatic dens fractures without subaxial fractures were identified, including 65 (22.8%) with simultaneous atlas fractures. The distribution of injury mechanisms differed between groups (χ2P = 0.0360). On multivariable logistic regression, dens nonunion was positively associated with type II fractures (odds ratio [OR] = 2.00, P = 0.038) and negatively associated with having surgery (OR = 0.52, P = 0.049), but not with having a C1 fracture (P = 0.3673). Worse myelopathy severity on presentation was associated with having a severe injury severity score (OR = 102.3, P < 0.001) and older age (OR = 1.28, P = 0.002), but not with having an atlas fracture (P = 0.2446). Having a simultaneous atlas fracture was associated with older age (OR = 1.29, P = 0.024) and dens fracture angulation (OR = 2.62, P = 0.004). Among patients who underwent surgery, C1/C2 posterior fusion was the most common procedure, and having a simultaneous atlas fracture was associated with selection for occipitocervical fusion (OCF) (OR = 14.35, P = 0.010).
Conclusions: Among patients with traumatic dens, patients who have simultaneous atlas fractures are a distinct subpopulation with respect to age, mechanism of injury, fracture morphology, and management. Traumatic dens fractures with simultaneous atlas fractures are independently associated with selection for OCF rather than posterior cervical fusion alone.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
