Patrick M Boland, John M L Ebos, Kristopher Attwood, Michalis Mastri, Christos Fountzilas, Renuka V Iyer, Christopher Banker, Andrew K L Goey, Robert Bies, Wen Wee Ma, Marwan Fakih
{"title":"宁替达尼和卡培他滨治疗难治性转移性结直肠癌的 I/II 期研究。","authors":"Patrick M Boland, John M L Ebos, Kristopher Attwood, Michalis Mastri, Christos Fountzilas, Renuka V Iyer, Christopher Banker, Andrew K L Goey, Robert Bies, Wen Wee Ma, Marwan Fakih","doi":"10.1093/jncics/pkae017","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Nintedanib is a tyrosine kinase inhibitor with efficacy in bevacizumab-resistant colorectal cancer models. This phase I/II study evaluated the recommended phase II dose and efficacy of nintedanib and capecitabine in refractory metastatic colorectal cancer.</p><p><strong>Methods: </strong>Key eligibility criteria included refractory metastatic colorectal cancer and ECOG performance status of 1 or lower. The primary endpoint was 18-week progression-free survival (PFS). A 1-sided binomial test (at α = .1) compared the observed 18-week PFS with a historic control of .25.</p><p><strong>Results: </strong>Forty-two patients were enrolled, including 39 at the recommended phase II dose. The recommended phase II dose was established to be nintedanib 200 mg by mouth twice daily and capecitabine 1000 mg/m2 by mouth twice daily. The protocol was evaluated for efficacy in 36 patients. The 18-week PFS was 42% (15/36 patients; P = .0209). Median PFS was 3.4 mo. Median overall survival was 8.9 mo. Sixteen (44%) patients experienced a grade 3/4 adverse event, most commonly fatigue (8%), palmoplantar erythrodysesthesia (8%), aspartate aminotransferase elevation (6%), asthenia (6%), pulmonary embolus (6%), and dehydration (6%). Osteopontin levels at cycle 1, day 1 and cycle 3, day 1 as well as ΔCCL2 levels correlated to disease control at 18 weeks.</p><p><strong>Conclusions: </strong>The combination of nintedanib and capecitabine is well tolerated. Clinical efficacy appears to be superior to regorafenib or tipiracil hydrochloride monotherapy. Further investigation of similar combinations is warranted.</p><p><strong>Clinicaltrials.gov identifier: </strong>NCT02393755.</p>","PeriodicalId":14681,"journal":{"name":"JNCI Cancer Spectrum","volume":"8 3","pages":""},"PeriodicalIF":4.8000,"publicationDate":"2024-04-30","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11065487/pdf/","citationCount":"0","resultStr":"{\"title\":\"A phase I/II study of nintedanib and capecitabine for refractory metastatic colorectal cancer.\",\"authors\":\"Patrick M Boland, John M L Ebos, Kristopher Attwood, Michalis Mastri, Christos Fountzilas, Renuka V Iyer, Christopher Banker, Andrew K L Goey, Robert Bies, Wen Wee Ma, Marwan Fakih\",\"doi\":\"10.1093/jncics/pkae017\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Nintedanib is a tyrosine kinase inhibitor with efficacy in bevacizumab-resistant colorectal cancer models. This phase I/II study evaluated the recommended phase II dose and efficacy of nintedanib and capecitabine in refractory metastatic colorectal cancer.</p><p><strong>Methods: </strong>Key eligibility criteria included refractory metastatic colorectal cancer and ECOG performance status of 1 or lower. The primary endpoint was 18-week progression-free survival (PFS). A 1-sided binomial test (at α = .1) compared the observed 18-week PFS with a historic control of .25.</p><p><strong>Results: </strong>Forty-two patients were enrolled, including 39 at the recommended phase II dose. The recommended phase II dose was established to be nintedanib 200 mg by mouth twice daily and capecitabine 1000 mg/m2 by mouth twice daily. The protocol was evaluated for efficacy in 36 patients. The 18-week PFS was 42% (15/36 patients; P = .0209). Median PFS was 3.4 mo. Median overall survival was 8.9 mo. Sixteen (44%) patients experienced a grade 3/4 adverse event, most commonly fatigue (8%), palmoplantar erythrodysesthesia (8%), aspartate aminotransferase elevation (6%), asthenia (6%), pulmonary embolus (6%), and dehydration (6%). Osteopontin levels at cycle 1, day 1 and cycle 3, day 1 as well as ΔCCL2 levels correlated to disease control at 18 weeks.</p><p><strong>Conclusions: </strong>The combination of nintedanib and capecitabine is well tolerated. Clinical efficacy appears to be superior to regorafenib or tipiracil hydrochloride monotherapy. Further investigation of similar combinations is warranted.</p><p><strong>Clinicaltrials.gov identifier: </strong>NCT02393755.</p>\",\"PeriodicalId\":14681,\"journal\":{\"name\":\"JNCI Cancer Spectrum\",\"volume\":\"8 3\",\"pages\":\"\"},\"PeriodicalIF\":4.8000,\"publicationDate\":\"2024-04-30\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11065487/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"JNCI Cancer Spectrum\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1093/jncics/pkae017\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q2\",\"JCRName\":\"ONCOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"JNCI Cancer Spectrum","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1093/jncics/pkae017","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"ONCOLOGY","Score":null,"Total":0}
A phase I/II study of nintedanib and capecitabine for refractory metastatic colorectal cancer.
Background: Nintedanib is a tyrosine kinase inhibitor with efficacy in bevacizumab-resistant colorectal cancer models. This phase I/II study evaluated the recommended phase II dose and efficacy of nintedanib and capecitabine in refractory metastatic colorectal cancer.
Methods: Key eligibility criteria included refractory metastatic colorectal cancer and ECOG performance status of 1 or lower. The primary endpoint was 18-week progression-free survival (PFS). A 1-sided binomial test (at α = .1) compared the observed 18-week PFS with a historic control of .25.
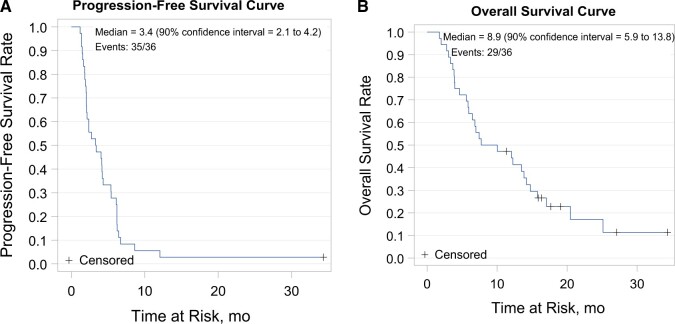
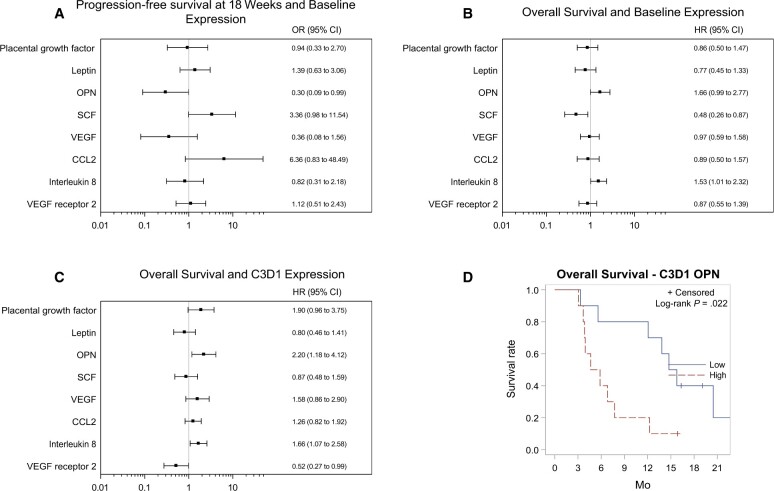
Results: Forty-two patients were enrolled, including 39 at the recommended phase II dose. The recommended phase II dose was established to be nintedanib 200 mg by mouth twice daily and capecitabine 1000 mg/m2 by mouth twice daily. The protocol was evaluated for efficacy in 36 patients. The 18-week PFS was 42% (15/36 patients; P = .0209). Median PFS was 3.4 mo. Median overall survival was 8.9 mo. Sixteen (44%) patients experienced a grade 3/4 adverse event, most commonly fatigue (8%), palmoplantar erythrodysesthesia (8%), aspartate aminotransferase elevation (6%), asthenia (6%), pulmonary embolus (6%), and dehydration (6%). Osteopontin levels at cycle 1, day 1 and cycle 3, day 1 as well as ΔCCL2 levels correlated to disease control at 18 weeks.
Conclusions: The combination of nintedanib and capecitabine is well tolerated. Clinical efficacy appears to be superior to regorafenib or tipiracil hydrochloride monotherapy. Further investigation of similar combinations is warranted.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
