Anthony Lau BSc(Pharm), PharmD, ACPR, Hans Haag BSc(Pharm), PharmD, ACPR, Anil Maharaj BSc(Pharm), PhD
{"title":"基于模拟的左乙拉西坦固定剂量和基于体重的负荷剂量浓度评估:元回归和药代动力学模型分析。","authors":"Anthony Lau BSc(Pharm), PharmD, ACPR, Hans Haag BSc(Pharm), PharmD, ACPR, Anil Maharaj BSc(Pharm), PhD","doi":"10.1002/jcph.2449","DOIUrl":null,"url":null,"abstract":"<p>Current recommendations for refractory status epilepticus (SE) unresponsive to benzodiazepines suggest a loading dose of levetiracetam (LEV) of 60 mg/kg to a maximum of 4500 mg. LEV therapeutic drug monitoring can help guide therapy and is garnering increasing attention. The objective of this study is to simulate the probability of target attainment (PTA) of fixed dose and weight-based loading doses of LEV with respect to established therapeutic target concentrations. Meta-regression of the current literature was performed to evaluate the relationship between intravenous LEV loading dose and seizure cessation in refractory SE patients. A previously published pharmacokinetic model was used to simulate the PTA capacity of competing single intravenous dosing schemes (fixed vs weight-based dosing) to achieve maximum (C<sub>peak</sub>) and 12-h (C<sub>12h</sub>) plasma concentrations that exceed 12 mg/L. The meta-regression indicated that dosage was not a statistically significant modulator of seizure control at dosages between 20 and 60 mg/kg. Stochastic simulations showed all dosing schemes achieved plasma C<sub>peak</sub> >12 mg/L, but C<sub>12h</sub> levels were <12 mg/L in subjects over 60 kg with a fixed dose ≤2000 mg or in subjects <60 kg with a weight-based dose <30 mg/kg. Dosages of 40 and 60 mg/kg provided ≥90% PTAs across all weights. Using a weight-based loading dose of 40 mg/kg, up to a suggested maximum of 4500 mg, improves the likelihood of achieving a sustained therapeutic drug concentration after the initial LEV dose, whereas fixed <3000 mg may not achieve the desired concentration before maintenance dosing.</p>","PeriodicalId":22751,"journal":{"name":"The Journal of Clinical Pharmacology","volume":"64 9","pages":"1173-1180"},"PeriodicalIF":0.0000,"publicationDate":"2024-05-06","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1002/jcph.2449","citationCount":"0","resultStr":"{\"title\":\"A Simulation-Based Assessment of Levetiracetam Concentrations Following Fixed and Weight-Based Loading Doses: A Meta-Regression and Pharmacokinetic Modeling Analysis\",\"authors\":\"Anthony Lau BSc(Pharm), PharmD, ACPR, Hans Haag BSc(Pharm), PharmD, ACPR, Anil Maharaj BSc(Pharm), PhD\",\"doi\":\"10.1002/jcph.2449\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p>Current recommendations for refractory status epilepticus (SE) unresponsive to benzodiazepines suggest a loading dose of levetiracetam (LEV) of 60 mg/kg to a maximum of 4500 mg. LEV therapeutic drug monitoring can help guide therapy and is garnering increasing attention. The objective of this study is to simulate the probability of target attainment (PTA) of fixed dose and weight-based loading doses of LEV with respect to established therapeutic target concentrations. Meta-regression of the current literature was performed to evaluate the relationship between intravenous LEV loading dose and seizure cessation in refractory SE patients. A previously published pharmacokinetic model was used to simulate the PTA capacity of competing single intravenous dosing schemes (fixed vs weight-based dosing) to achieve maximum (C<sub>peak</sub>) and 12-h (C<sub>12h</sub>) plasma concentrations that exceed 12 mg/L. The meta-regression indicated that dosage was not a statistically significant modulator of seizure control at dosages between 20 and 60 mg/kg. Stochastic simulations showed all dosing schemes achieved plasma C<sub>peak</sub> >12 mg/L, but C<sub>12h</sub> levels were <12 mg/L in subjects over 60 kg with a fixed dose ≤2000 mg or in subjects <60 kg with a weight-based dose <30 mg/kg. Dosages of 40 and 60 mg/kg provided ≥90% PTAs across all weights. Using a weight-based loading dose of 40 mg/kg, up to a suggested maximum of 4500 mg, improves the likelihood of achieving a sustained therapeutic drug concentration after the initial LEV dose, whereas fixed <3000 mg may not achieve the desired concentration before maintenance dosing.</p>\",\"PeriodicalId\":22751,\"journal\":{\"name\":\"The Journal of Clinical Pharmacology\",\"volume\":\"64 9\",\"pages\":\"1173-1180\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2024-05-06\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://onlinelibrary.wiley.com/doi/epdf/10.1002/jcph.2449\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"The Journal of Clinical Pharmacology\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://accp1.onlinelibrary.wiley.com/doi/10.1002/jcph.2449\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"The Journal of Clinical Pharmacology","FirstCategoryId":"1085","ListUrlMain":"https://accp1.onlinelibrary.wiley.com/doi/10.1002/jcph.2449","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
摘要
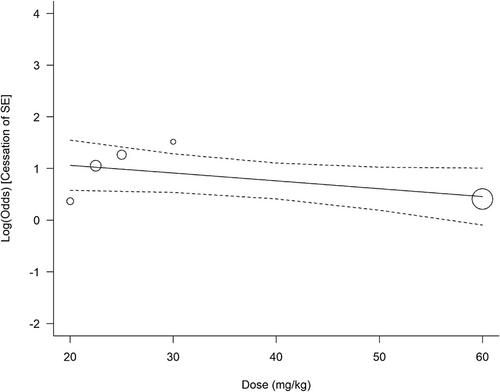
针对对苯二氮卓类药物无反应的难治性癫痫状态(SE),目前的建议是,左乙拉西坦(LEV)的负荷剂量为 60 毫克/千克,最大剂量为 4500 毫克。左乙拉西坦治疗药物监测可帮助指导治疗,正受到越来越多的关注。本研究旨在模拟 LEV 固定剂量和基于体重的负荷剂量达到既定治疗目标浓度的概率(PTA)。我们对现有文献进行了元回归,以评估难治性 SE 患者静脉注射 LEV 负荷剂量与癫痫发作停止之间的关系。研究人员使用以前发表的药代动力学模型模拟了相互竞争的单一静脉给药方案(固定给药与按体重给药)的 PTA 能力,以达到超过 12 毫克/升的最大(Cpeak)和 12 小时(C12h)血浆浓度。元回归结果表明,在 20 至 60 毫克/千克的剂量范围内,剂量对癫痫发作控制的调节作用不具有统计学意义。随机模拟显示,所有给药方案都能使血浆 Cpeak 浓度大于 12 毫克/升,但 C12h 浓度低于 12 毫克/升。
A Simulation-Based Assessment of Levetiracetam Concentrations Following Fixed and Weight-Based Loading Doses: A Meta-Regression and Pharmacokinetic Modeling Analysis
Current recommendations for refractory status epilepticus (SE) unresponsive to benzodiazepines suggest a loading dose of levetiracetam (LEV) of 60 mg/kg to a maximum of 4500 mg. LEV therapeutic drug monitoring can help guide therapy and is garnering increasing attention. The objective of this study is to simulate the probability of target attainment (PTA) of fixed dose and weight-based loading doses of LEV with respect to established therapeutic target concentrations. Meta-regression of the current literature was performed to evaluate the relationship between intravenous LEV loading dose and seizure cessation in refractory SE patients. A previously published pharmacokinetic model was used to simulate the PTA capacity of competing single intravenous dosing schemes (fixed vs weight-based dosing) to achieve maximum (Cpeak) and 12-h (C12h) plasma concentrations that exceed 12 mg/L. The meta-regression indicated that dosage was not a statistically significant modulator of seizure control at dosages between 20 and 60 mg/kg. Stochastic simulations showed all dosing schemes achieved plasma Cpeak >12 mg/L, but C12h levels were <12 mg/L in subjects over 60 kg with a fixed dose ≤2000 mg or in subjects <60 kg with a weight-based dose <30 mg/kg. Dosages of 40 and 60 mg/kg provided ≥90% PTAs across all weights. Using a weight-based loading dose of 40 mg/kg, up to a suggested maximum of 4500 mg, improves the likelihood of achieving a sustained therapeutic drug concentration after the initial LEV dose, whereas fixed <3000 mg may not achieve the desired concentration before maintenance dosing.




 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
