Luca Sorrentino, Andrea Scardino, Luigi Battaglia, Raffaella Vigorito, Giovanna Sabella, Filippo Patti, Michele Prisciandaro, Elena Daveri, Alessandro Gronchi, Filiberto Belli, Marcello Guaglio
{"title":"化疗/放疗 vs. R2手术切除 vs. 姑息治疗对非切除性局部复发性直肠癌的疗效。","authors":"Luca Sorrentino, Andrea Scardino, Luigi Battaglia, Raffaella Vigorito, Giovanna Sabella, Filippo Patti, Michele Prisciandaro, Elena Daveri, Alessandro Gronchi, Filiberto Belli, Marcello Guaglio","doi":"10.1177/03008916241253130","DOIUrl":null,"url":null,"abstract":"<p><p>Locally recurrent rectal cancer is resected with clear margins in only 50% of cases, and these patients achieve a three-year survival rate of 50%. Outcomes and therapeutic strategies for nonresectable locally recurrent rectal cancer have been much less explored. The aim of the study was to assess the three-year progression-free survival and the three-year overall survival in locally recurrent rectal cancer patients treated by chemotherapy/chemoradiation only vs. chemotherapy/chemoradiation and R2 surgical debulking vs. palliative care. A total of 86 patients affected by nonresectable locally recurrent rectal cancer were included: three-year progression-free survival was 15.8% with chemotherapy/chemoradiation vs. 20.3% with R2 surgical debulking (Log-rank p=0.567), but both rates were higher than best palliative care (0.0%, Log-rank p=0.0004). Three-year overall survival rates were respectively 62.0%, 70.8% and 0.0% (Log-rank p<0.0001). Chemotherapy/chemoradiation (HR 0.33, p=0.028) and R2 surgical debulking with or without chemotherapy/chemoradiation (HR 0.23, p=0.005) were independent predictors of improved progression-free survival on multivariate analysis. In conclusion, both chemotherapy/chemoradiation alone and R2 surgery with or without chemotherapy/chemoradiation provide a survival benefit over palliative care in nonresectable locally recurrent rectal cancer. However, considering that pelvic debulking is burdened by a high rate of complications, and considering its negligible impact on progression-free survival and overall survival when associated to medical therapy, surgery should be avoided in this setting.</p>","PeriodicalId":23349,"journal":{"name":"Tumori","volume":" ","pages":"360-365"},"PeriodicalIF":3.1000,"publicationDate":"2024-10-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11459869/pdf/","citationCount":"0","resultStr":"{\"title\":\"Outcomes of chemotherapy/chemoradiation vs. R2 surgical debulking vs. palliative care in nonresectable locally recurrent rectal cancer.\",\"authors\":\"Luca Sorrentino, Andrea Scardino, Luigi Battaglia, Raffaella Vigorito, Giovanna Sabella, Filippo Patti, Michele Prisciandaro, Elena Daveri, Alessandro Gronchi, Filiberto Belli, Marcello Guaglio\",\"doi\":\"10.1177/03008916241253130\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>Locally recurrent rectal cancer is resected with clear margins in only 50% of cases, and these patients achieve a three-year survival rate of 50%. Outcomes and therapeutic strategies for nonresectable locally recurrent rectal cancer have been much less explored. The aim of the study was to assess the three-year progression-free survival and the three-year overall survival in locally recurrent rectal cancer patients treated by chemotherapy/chemoradiation only vs. chemotherapy/chemoradiation and R2 surgical debulking vs. palliative care. A total of 86 patients affected by nonresectable locally recurrent rectal cancer were included: three-year progression-free survival was 15.8% with chemotherapy/chemoradiation vs. 20.3% with R2 surgical debulking (Log-rank p=0.567), but both rates were higher than best palliative care (0.0%, Log-rank p=0.0004). Three-year overall survival rates were respectively 62.0%, 70.8% and 0.0% (Log-rank p<0.0001). Chemotherapy/chemoradiation (HR 0.33, p=0.028) and R2 surgical debulking with or without chemotherapy/chemoradiation (HR 0.23, p=0.005) were independent predictors of improved progression-free survival on multivariate analysis. In conclusion, both chemotherapy/chemoradiation alone and R2 surgery with or without chemotherapy/chemoradiation provide a survival benefit over palliative care in nonresectable locally recurrent rectal cancer. However, considering that pelvic debulking is burdened by a high rate of complications, and considering its negligible impact on progression-free survival and overall survival when associated to medical therapy, surgery should be avoided in this setting.</p>\",\"PeriodicalId\":23349,\"journal\":{\"name\":\"Tumori\",\"volume\":\" \",\"pages\":\"360-365\"},\"PeriodicalIF\":3.1000,\"publicationDate\":\"2024-10-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11459869/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Tumori\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1177/03008916241253130\",\"RegionNum\":4,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2024/5/10 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q3\",\"JCRName\":\"ONCOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Tumori","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1177/03008916241253130","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/5/10 0:00:00","PubModel":"Epub","JCR":"Q3","JCRName":"ONCOLOGY","Score":null,"Total":0}
Outcomes of chemotherapy/chemoradiation vs. R2 surgical debulking vs. palliative care in nonresectable locally recurrent rectal cancer.
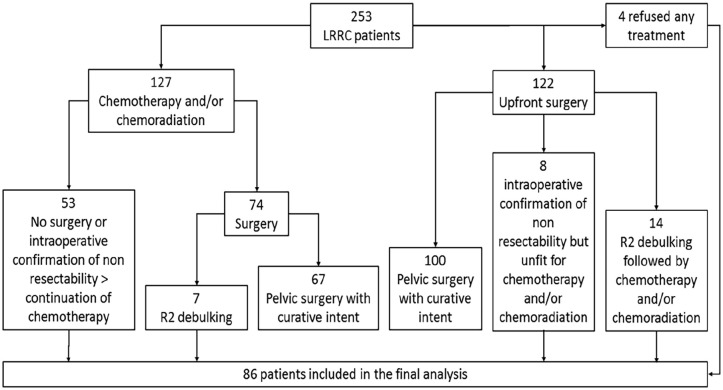
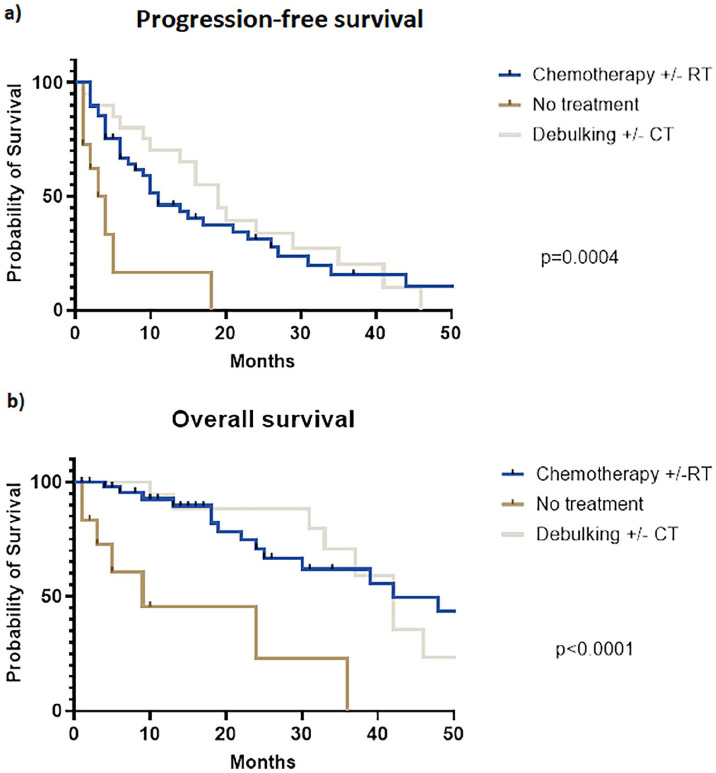
Locally recurrent rectal cancer is resected with clear margins in only 50% of cases, and these patients achieve a three-year survival rate of 50%. Outcomes and therapeutic strategies for nonresectable locally recurrent rectal cancer have been much less explored. The aim of the study was to assess the three-year progression-free survival and the three-year overall survival in locally recurrent rectal cancer patients treated by chemotherapy/chemoradiation only vs. chemotherapy/chemoradiation and R2 surgical debulking vs. palliative care. A total of 86 patients affected by nonresectable locally recurrent rectal cancer were included: three-year progression-free survival was 15.8% with chemotherapy/chemoradiation vs. 20.3% with R2 surgical debulking (Log-rank p=0.567), but both rates were higher than best palliative care (0.0%, Log-rank p=0.0004). Three-year overall survival rates were respectively 62.0%, 70.8% and 0.0% (Log-rank p<0.0001). Chemotherapy/chemoradiation (HR 0.33, p=0.028) and R2 surgical debulking with or without chemotherapy/chemoradiation (HR 0.23, p=0.005) were independent predictors of improved progression-free survival on multivariate analysis. In conclusion, both chemotherapy/chemoradiation alone and R2 surgery with or without chemotherapy/chemoradiation provide a survival benefit over palliative care in nonresectable locally recurrent rectal cancer. However, considering that pelvic debulking is burdened by a high rate of complications, and considering its negligible impact on progression-free survival and overall survival when associated to medical therapy, surgery should be avoided in this setting.
期刊介绍:
Tumori Journal covers all aspects of cancer science and clinical practice with a strong focus on prevention, translational medicine and clinically relevant reports. We invite the publication of randomized trials and reports on large, consecutive patient series that investigate the real impact of new techniques, drugs and devices inday-to-day clinical practice.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
