Jessica L. Markham MD, MSc, Alaina Burns PharmD, BCPPS, Matthew Hall PhD, Matthew J. Molloy MD, MPH, John R. Stephens MD, Elisha McCoy MD, Irma T. Ugalde MD, MBE, Michael J. Steiner MD, MPH, Jillian M. Cotter MD, MSCS, Samantha A. House DO, MPH, Megan E. Collins MD, Andrew G. Yu MD, Michael J. Tchou MD, MSc, Samir S. Shah MD, MSCE
{"title":"泌尿道感染住院患儿初始使用窄谱抗生素与广谱抗生素的相关结果。","authors":"Jessica L. Markham MD, MSc, Alaina Burns PharmD, BCPPS, Matthew Hall PhD, Matthew J. Molloy MD, MPH, John R. Stephens MD, Elisha McCoy MD, Irma T. Ugalde MD, MBE, Michael J. Steiner MD, MPH, Jillian M. Cotter MD, MSCS, Samantha A. House DO, MPH, Megan E. Collins MD, Andrew G. Yu MD, Michael J. Tchou MD, MSc, Samir S. Shah MD, MSCE","doi":"10.1002/jhm.13390","DOIUrl":null,"url":null,"abstract":"<div>\n \n \n <section>\n \n <h3> Objective</h3>\n \n <p>The aim of this study is to describe the proportion of children hospitalized with urinary tract infections (UTIs) who receive initial narrow- versus broad-spectrum antibiotics across children's hospitals and explore whether the use of initial narrow-spectrum antibiotics is associated with different outcomes.</p>\n </section>\n \n <section>\n \n <h3> Design, Setting and Participants</h3>\n \n <p>We performed a retrospective cohort analysis of children aged 2 months to 17 years hospitalized with UTI (inclusive of pyelonephritis) using the Pediatric Health Information System (PHIS) database.</p>\n </section>\n \n <section>\n \n <h3> Main Outcome and Measures</h3>\n \n <p>We analyzed the proportions of children initially receiving narrow- versus broad-spectrum antibiotics; additionally, we compiled antibiogram data for common uropathogenic organisms from participating hospitals to compare with the observed antibiotic susceptibility patterns. We examined the association of antibiotic type with adjusted outcomes including length of stay (LOS), costs, and 7- and 30-day emergency department (ED) revisits and hospital readmissions.</p>\n </section>\n \n <section>\n \n <h3> Results</h3>\n \n <p>We identified 10,740 hospitalizations for UTI across 39 hospitals. Approximately 5% of encounters demonstrated initial narrow-spectrum antibiotics, with hospital-level narrow-spectrum use ranging from <1% to 25%. Approximately 80% of hospital antibiograms demonstrated >80% <i>Escherichia coli</i> susceptibility to cefazolin. In adjusted models, those who received initial narrow-spectrum antibiotics had shorter LOS (narrow-spectrum: 33.1 [95% confidence interval; CI]: 30.8–35.4] h vs. broad-spectrum: 46.1 [95% CI: 44.1–48.2] h) and reduced costs (narrow-spectrum: $4570 [$3751–5568] versus broad-spectrum: $5699 [$5005–$6491]). There were no differences in ED revisits or hospital readmissions. In summary, children's hospitals have low rates of narrow-spectrum antibiotic use for UTIs despite many reporting high rates of cefazolin-susceptible <i>E. coli</i>. These findings, coupled with the observed decreased LOS and costs among those receiving narrow-spectrum antibiotics, highlight potential antibiotic stewardship opportunities.</p>\n </section>\n </div>","PeriodicalId":15883,"journal":{"name":"Journal of hospital medicine","volume":"19 9","pages":"777-786"},"PeriodicalIF":2.3000,"publicationDate":"2024-05-12","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"","citationCount":"0","resultStr":"{\"title\":\"Outcomes associated with initial narrow-spectrum versus broad-spectrum antibiotics in children hospitalized with urinary tract infections\",\"authors\":\"Jessica L. Markham MD, MSc, Alaina Burns PharmD, BCPPS, Matthew Hall PhD, Matthew J. Molloy MD, MPH, John R. Stephens MD, Elisha McCoy MD, Irma T. Ugalde MD, MBE, Michael J. Steiner MD, MPH, Jillian M. Cotter MD, MSCS, Samantha A. House DO, MPH, Megan E. Collins MD, Andrew G. Yu MD, Michael J. Tchou MD, MSc, Samir S. Shah MD, MSCE\",\"doi\":\"10.1002/jhm.13390\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<div>\\n \\n \\n <section>\\n \\n <h3> Objective</h3>\\n \\n <p>The aim of this study is to describe the proportion of children hospitalized with urinary tract infections (UTIs) who receive initial narrow- versus broad-spectrum antibiotics across children's hospitals and explore whether the use of initial narrow-spectrum antibiotics is associated with different outcomes.</p>\\n </section>\\n \\n <section>\\n \\n <h3> Design, Setting and Participants</h3>\\n \\n <p>We performed a retrospective cohort analysis of children aged 2 months to 17 years hospitalized with UTI (inclusive of pyelonephritis) using the Pediatric Health Information System (PHIS) database.</p>\\n </section>\\n \\n <section>\\n \\n <h3> Main Outcome and Measures</h3>\\n \\n <p>We analyzed the proportions of children initially receiving narrow- versus broad-spectrum antibiotics; additionally, we compiled antibiogram data for common uropathogenic organisms from participating hospitals to compare with the observed antibiotic susceptibility patterns. We examined the association of antibiotic type with adjusted outcomes including length of stay (LOS), costs, and 7- and 30-day emergency department (ED) revisits and hospital readmissions.</p>\\n </section>\\n \\n <section>\\n \\n <h3> Results</h3>\\n \\n <p>We identified 10,740 hospitalizations for UTI across 39 hospitals. Approximately 5% of encounters demonstrated initial narrow-spectrum antibiotics, with hospital-level narrow-spectrum use ranging from <1% to 25%. Approximately 80% of hospital antibiograms demonstrated >80% <i>Escherichia coli</i> susceptibility to cefazolin. In adjusted models, those who received initial narrow-spectrum antibiotics had shorter LOS (narrow-spectrum: 33.1 [95% confidence interval; CI]: 30.8–35.4] h vs. broad-spectrum: 46.1 [95% CI: 44.1–48.2] h) and reduced costs (narrow-spectrum: $4570 [$3751–5568] versus broad-spectrum: $5699 [$5005–$6491]). There were no differences in ED revisits or hospital readmissions. In summary, children's hospitals have low rates of narrow-spectrum antibiotic use for UTIs despite many reporting high rates of cefazolin-susceptible <i>E. coli</i>. These findings, coupled with the observed decreased LOS and costs among those receiving narrow-spectrum antibiotics, highlight potential antibiotic stewardship opportunities.</p>\\n </section>\\n </div>\",\"PeriodicalId\":15883,\"journal\":{\"name\":\"Journal of hospital medicine\",\"volume\":\"19 9\",\"pages\":\"777-786\"},\"PeriodicalIF\":2.3000,\"publicationDate\":\"2024-05-12\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of hospital medicine\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://shmpublications.onlinelibrary.wiley.com/doi/10.1002/jhm.13390\",\"RegionNum\":4,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q1\",\"JCRName\":\"MEDICINE, GENERAL & INTERNAL\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of hospital medicine","FirstCategoryId":"3","ListUrlMain":"https://shmpublications.onlinelibrary.wiley.com/doi/10.1002/jhm.13390","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"MEDICINE, GENERAL & INTERNAL","Score":null,"Total":0}
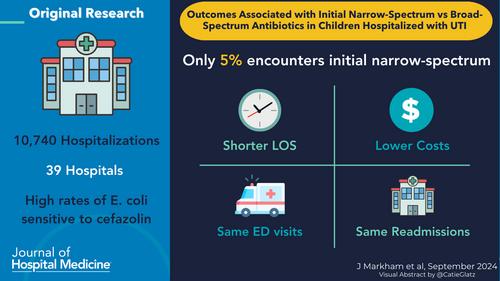
Outcomes associated with initial narrow-spectrum versus broad-spectrum antibiotics in children hospitalized with urinary tract infections
Objective
The aim of this study is to describe the proportion of children hospitalized with urinary tract infections (UTIs) who receive initial narrow- versus broad-spectrum antibiotics across children's hospitals and explore whether the use of initial narrow-spectrum antibiotics is associated with different outcomes.
Design, Setting and Participants
We performed a retrospective cohort analysis of children aged 2 months to 17 years hospitalized with UTI (inclusive of pyelonephritis) using the Pediatric Health Information System (PHIS) database.
Main Outcome and Measures
We analyzed the proportions of children initially receiving narrow- versus broad-spectrum antibiotics; additionally, we compiled antibiogram data for common uropathogenic organisms from participating hospitals to compare with the observed antibiotic susceptibility patterns. We examined the association of antibiotic type with adjusted outcomes including length of stay (LOS), costs, and 7- and 30-day emergency department (ED) revisits and hospital readmissions.
Results
We identified 10,740 hospitalizations for UTI across 39 hospitals. Approximately 5% of encounters demonstrated initial narrow-spectrum antibiotics, with hospital-level narrow-spectrum use ranging from <1% to 25%. Approximately 80% of hospital antibiograms demonstrated >80% Escherichia coli susceptibility to cefazolin. In adjusted models, those who received initial narrow-spectrum antibiotics had shorter LOS (narrow-spectrum: 33.1 [95% confidence interval; CI]: 30.8–35.4] h vs. broad-spectrum: 46.1 [95% CI: 44.1–48.2] h) and reduced costs (narrow-spectrum: $4570 [$3751–5568] versus broad-spectrum: $5699 [$5005–$6491]). There were no differences in ED revisits or hospital readmissions. In summary, children's hospitals have low rates of narrow-spectrum antibiotic use for UTIs despite many reporting high rates of cefazolin-susceptible E. coli. These findings, coupled with the observed decreased LOS and costs among those receiving narrow-spectrum antibiotics, highlight potential antibiotic stewardship opportunities.
期刊介绍:
JHM is a peer-reviewed publication of the Society of Hospital Medicine and is published 12 times per year. JHM publishes manuscripts that address the care of hospitalized adults or children.
Broad areas of interest include (1) Treatments for common inpatient conditions; (2) Approaches to improving perioperative care; (3) Improving care for hospitalized patients with geriatric or pediatric vulnerabilities (such as mobility problems, or those with complex longitudinal care); (4) Evaluation of innovative healthcare delivery or educational models; (5) Approaches to improving the quality, safety, and value of healthcare across the acute- and postacute-continuum of care; and (6) Evaluation of policy and payment changes that affect hospital and postacute care.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
