Ali H Alassiri, Turki M Alfayea, Tariq I Aljared, Khaled R Alenezi
{"title":"散发性巨细胞星形细胞瘤伴有体细胞TSC2突变:病例报告。","authors":"Ali H Alassiri, Turki M Alfayea, Tariq I Aljared, Khaled R Alenezi","doi":"10.17712/nsj.2024.2.20230089","DOIUrl":null,"url":null,"abstract":"<p><p>Subependymal giant cell astrocytoma (SEGA) is a rare circumscribed astrocytic glioma that occurs in approximately 25% of all tuberous sclerosis (TSC) cases. Herein, we discuss an atypical presentation of SEGA, including the genetic alterations, impact on clinical presentation, and the determinants of each medical and surgical treatment option. A 14-year-old girl presented with intermittent headache and a right intraventricular mass originating near the foramen of Monro. The tumor's proximity to critical structures necessitated maximum safe resection, which improved her symptoms. Histological findings indicated SEGA, and genetic sequencing revealed a <i>TSC2</i> mutation. However, complete clinical and radiological evaluations failed to reveal TSC. Two months later, a new subependymal nodule was incidentally found. She had a recurrent left occipital horn lesion and diffuse smooth leptomeningeal enhancement with no spine drop metastases. She was administered everolimus as the tumor was considered unresectable. Subsequent imaging revealed a reduction in both residual and new lesions.</p>","PeriodicalId":19284,"journal":{"name":"Neurosciences","volume":"29 2","pages":"139-143"},"PeriodicalIF":1.3000,"publicationDate":"2024-05-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11305366/pdf/","citationCount":"0","resultStr":"{\"title\":\"Sporadic subependymal giant cell astrocytoma with somatic <i>TSC2</i> mutation: A case report.\",\"authors\":\"Ali H Alassiri, Turki M Alfayea, Tariq I Aljared, Khaled R Alenezi\",\"doi\":\"10.17712/nsj.2024.2.20230089\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>Subependymal giant cell astrocytoma (SEGA) is a rare circumscribed astrocytic glioma that occurs in approximately 25% of all tuberous sclerosis (TSC) cases. Herein, we discuss an atypical presentation of SEGA, including the genetic alterations, impact on clinical presentation, and the determinants of each medical and surgical treatment option. A 14-year-old girl presented with intermittent headache and a right intraventricular mass originating near the foramen of Monro. The tumor's proximity to critical structures necessitated maximum safe resection, which improved her symptoms. Histological findings indicated SEGA, and genetic sequencing revealed a <i>TSC2</i> mutation. However, complete clinical and radiological evaluations failed to reveal TSC. Two months later, a new subependymal nodule was incidentally found. She had a recurrent left occipital horn lesion and diffuse smooth leptomeningeal enhancement with no spine drop metastases. She was administered everolimus as the tumor was considered unresectable. Subsequent imaging revealed a reduction in both residual and new lesions.</p>\",\"PeriodicalId\":19284,\"journal\":{\"name\":\"Neurosciences\",\"volume\":\"29 2\",\"pages\":\"139-143\"},\"PeriodicalIF\":1.3000,\"publicationDate\":\"2024-05-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11305366/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Neurosciences\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.17712/nsj.2024.2.20230089\",\"RegionNum\":4,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q4\",\"JCRName\":\"CLINICAL NEUROLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Neurosciences","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.17712/nsj.2024.2.20230089","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q4","JCRName":"CLINICAL NEUROLOGY","Score":null,"Total":0}
引用次数: 0
摘要
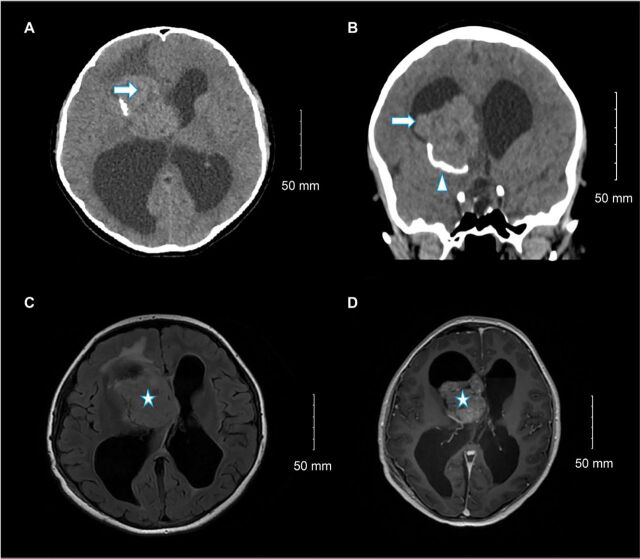
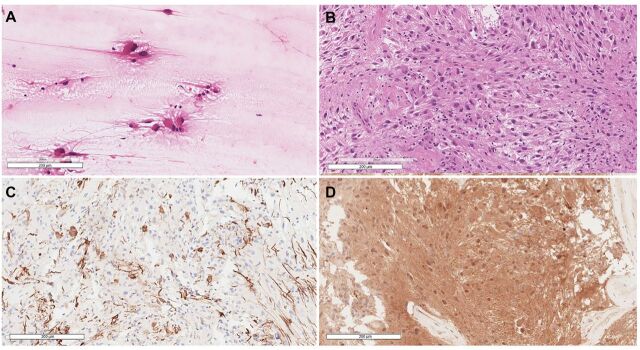
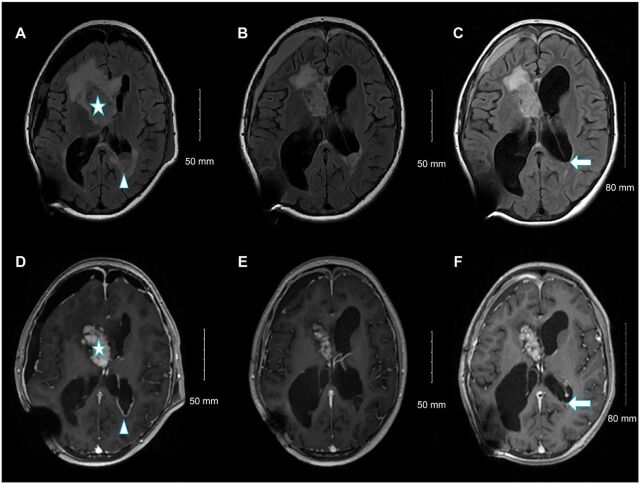
脐下巨细胞星形细胞瘤(SEGA)是一种罕见的环形星形胶质瘤,约占结节性硬化症(TSC)病例的25%。在此,我们将讨论 SEGA 的一种非典型表现,包括遗传改变、对临床表现的影响以及每种药物和手术治疗方案的决定因素。一名14岁的女孩因间歇性头痛和右侧脑室内肿块(起源于门罗孔附近)而就诊。由于肿瘤靠近重要结构,必须进行最大限度的安全切除,这才改善了她的症状。组织学检查结果显示她患有SEGA,基因测序显示她有TSC2基因突变。然而,完整的临床和放射学评估未能发现 TSC。两个月后,偶然发现了一个新的蝶鞍下结节。她的左枕角病变复发,弥漫性平滑脑膜强化,无脊柱下垂转移。由于肿瘤无法切除,她接受了依维莫司治疗。随后的影像学检查显示,残留病灶和新发病灶均有所减少。
Sporadic subependymal giant cell astrocytoma with somatic TSC2 mutation: A case report.
Subependymal giant cell astrocytoma (SEGA) is a rare circumscribed astrocytic glioma that occurs in approximately 25% of all tuberous sclerosis (TSC) cases. Herein, we discuss an atypical presentation of SEGA, including the genetic alterations, impact on clinical presentation, and the determinants of each medical and surgical treatment option. A 14-year-old girl presented with intermittent headache and a right intraventricular mass originating near the foramen of Monro. The tumor's proximity to critical structures necessitated maximum safe resection, which improved her symptoms. Histological findings indicated SEGA, and genetic sequencing revealed a TSC2 mutation. However, complete clinical and radiological evaluations failed to reveal TSC. Two months later, a new subependymal nodule was incidentally found. She had a recurrent left occipital horn lesion and diffuse smooth leptomeningeal enhancement with no spine drop metastases. She was administered everolimus as the tumor was considered unresectable. Subsequent imaging revealed a reduction in both residual and new lesions.
期刊介绍:
Neurosciences is an open access, peer-reviewed, quarterly publication. Authors are invited to submit for publication articles reporting original work related to the nervous system, e.g., neurology, neurophysiology, neuroradiology, neurosurgery, neurorehabilitation, neurooncology, neuropsychiatry, and neurogenetics, etc. Basic research withclear clinical implications will also be considered. Review articles of current interest and high standard are welcomed for consideration. Prospective workshould not be backdated. There are also sections for Case Reports, Brief Communication, Correspondence, and medical news items. To promote continuous education, training, and learning, we include Clinical Images and MCQ’s. Highlights of international and regional meetings of interest, and specialized supplements will also be considered. All submissions must conform to the Uniform Requirements.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
