A Teshon, R Reyes, D P Schammel, O Corso, C Schammel, P Kent, A M Devane
{"title":"念珠菌和放线菌合并感染引起的气管食管瘘:病例报告和文献综述。","authors":"A Teshon, R Reyes, D P Schammel, O Corso, C Schammel, P Kent, A M Devane","doi":"10.1556/1886.2024.00043","DOIUrl":null,"url":null,"abstract":"<p><p>Acquired benign tracheoesophageal fistulas and bronchoesophageal fistulas (TEF) are typically associated with granulomatous mediastinal infections, 75% of which are iatrogenic. Candida albicans and Actinomyces are commonly occurring organisms, but are uncommon etiologies of TEF. Normal colonization and the slow growth characteristics of some species of these agents rarely result in infection, mycetoma, and broncholithiasis, and thus, delays in diagnosis and treatment are likely. Few reports describe C. albicans or Actinomyces spp. as the etiology of TEF or broncholithiasis. Herein, we report a case of benign acquired TEF secondary to coinfection of Candida and Actinomyces complicated by the formation of an actinomycetoma and broncholithiasis and a comprehensive literature review to highlight the unique nature of this presentation and offer a diagnostic algorithm for diagnosis and treatment of TEFs. Following a presentation of three months of productive cough, choking sensation, night sweats, and weight loss, a bronchoscopy revealed a fistulous connection between the esophagus and the posterior right middle lobe. Pathology identified a calcified fungus ball and a broncholith secondary to the co-infection of Candida and Actinomyces. This unique presentation of Candida and Actinomyces co-infection and the associated diagnostic algorithm are presented as education and a useful tool for clinicians.</p>","PeriodicalId":93998,"journal":{"name":"European journal of microbiology & immunology","volume":" ","pages":"296-307"},"PeriodicalIF":0.0000,"publicationDate":"2024-05-13","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11393647/pdf/","citationCount":"0","resultStr":"{\"title\":\"Tracheoesophageal fistula due to Candida and Actinomyces co-infection: A case report and comprehensive review of the literature.\",\"authors\":\"A Teshon, R Reyes, D P Schammel, O Corso, C Schammel, P Kent, A M Devane\",\"doi\":\"10.1556/1886.2024.00043\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>Acquired benign tracheoesophageal fistulas and bronchoesophageal fistulas (TEF) are typically associated with granulomatous mediastinal infections, 75% of which are iatrogenic. Candida albicans and Actinomyces are commonly occurring organisms, but are uncommon etiologies of TEF. Normal colonization and the slow growth characteristics of some species of these agents rarely result in infection, mycetoma, and broncholithiasis, and thus, delays in diagnosis and treatment are likely. Few reports describe C. albicans or Actinomyces spp. as the etiology of TEF or broncholithiasis. Herein, we report a case of benign acquired TEF secondary to coinfection of Candida and Actinomyces complicated by the formation of an actinomycetoma and broncholithiasis and a comprehensive literature review to highlight the unique nature of this presentation and offer a diagnostic algorithm for diagnosis and treatment of TEFs. Following a presentation of three months of productive cough, choking sensation, night sweats, and weight loss, a bronchoscopy revealed a fistulous connection between the esophagus and the posterior right middle lobe. Pathology identified a calcified fungus ball and a broncholith secondary to the co-infection of Candida and Actinomyces. This unique presentation of Candida and Actinomyces co-infection and the associated diagnostic algorithm are presented as education and a useful tool for clinicians.</p>\",\"PeriodicalId\":93998,\"journal\":{\"name\":\"European journal of microbiology & immunology\",\"volume\":\" \",\"pages\":\"296-307\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2024-05-13\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11393647/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"European journal of microbiology & immunology\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1556/1886.2024.00043\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2024/9/11 0:00:00\",\"PubModel\":\"Print\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"European journal of microbiology & immunology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1556/1886.2024.00043","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/9/11 0:00:00","PubModel":"Print","JCR":"","JCRName":"","Score":null,"Total":0}
Tracheoesophageal fistula due to Candida and Actinomyces co-infection: A case report and comprehensive review of the literature.
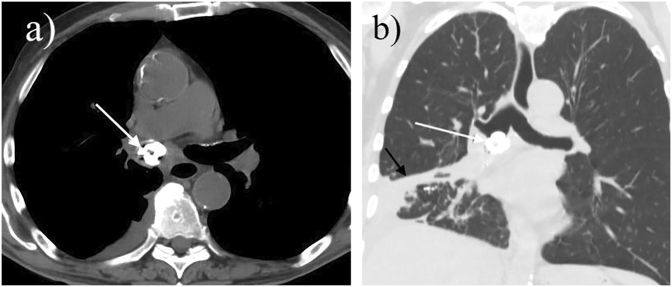
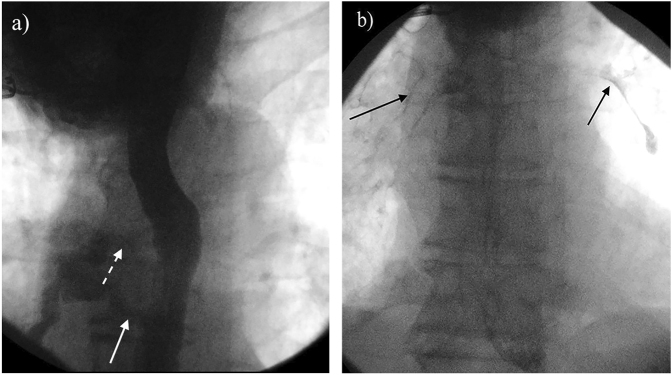
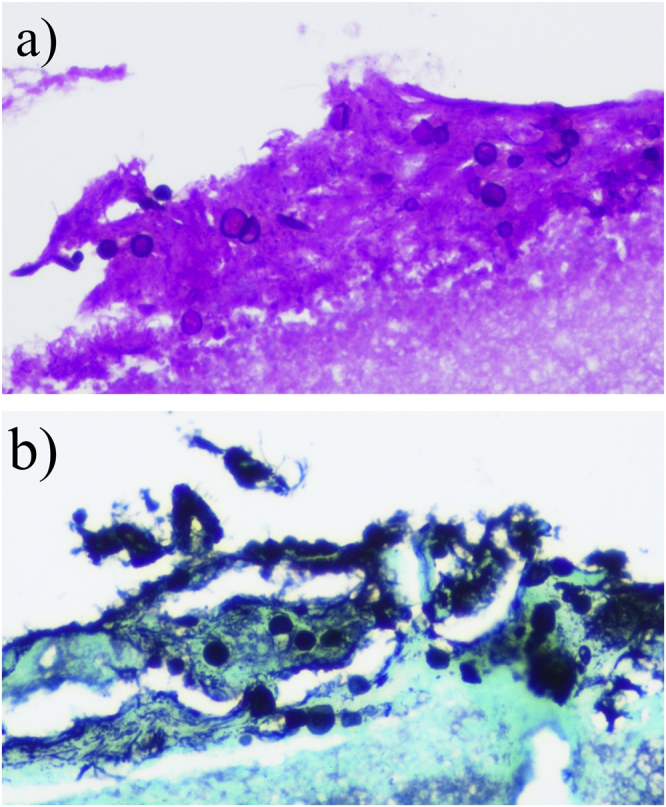
Acquired benign tracheoesophageal fistulas and bronchoesophageal fistulas (TEF) are typically associated with granulomatous mediastinal infections, 75% of which are iatrogenic. Candida albicans and Actinomyces are commonly occurring organisms, but are uncommon etiologies of TEF. Normal colonization and the slow growth characteristics of some species of these agents rarely result in infection, mycetoma, and broncholithiasis, and thus, delays in diagnosis and treatment are likely. Few reports describe C. albicans or Actinomyces spp. as the etiology of TEF or broncholithiasis. Herein, we report a case of benign acquired TEF secondary to coinfection of Candida and Actinomyces complicated by the formation of an actinomycetoma and broncholithiasis and a comprehensive literature review to highlight the unique nature of this presentation and offer a diagnostic algorithm for diagnosis and treatment of TEFs. Following a presentation of three months of productive cough, choking sensation, night sweats, and weight loss, a bronchoscopy revealed a fistulous connection between the esophagus and the posterior right middle lobe. Pathology identified a calcified fungus ball and a broncholith secondary to the co-infection of Candida and Actinomyces. This unique presentation of Candida and Actinomyces co-infection and the associated diagnostic algorithm are presented as education and a useful tool for clinicians.



 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
