Jaehong Kim, Shanshan Wang, Slaven Sikirica, Jason Shafrin
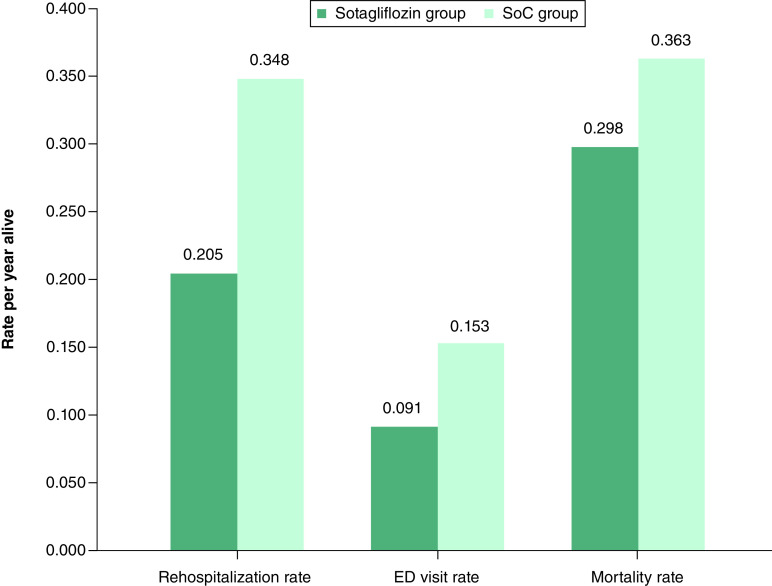
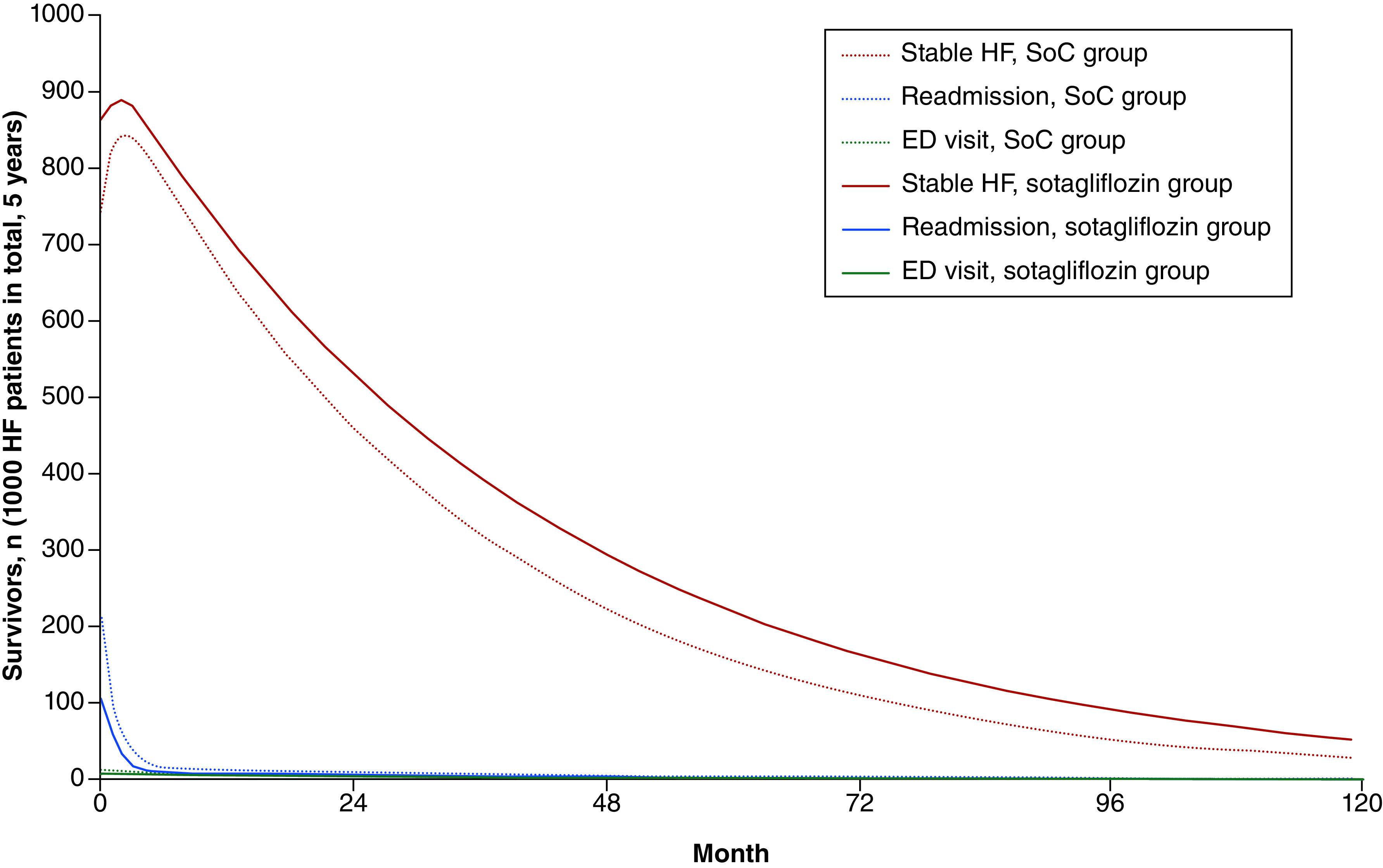
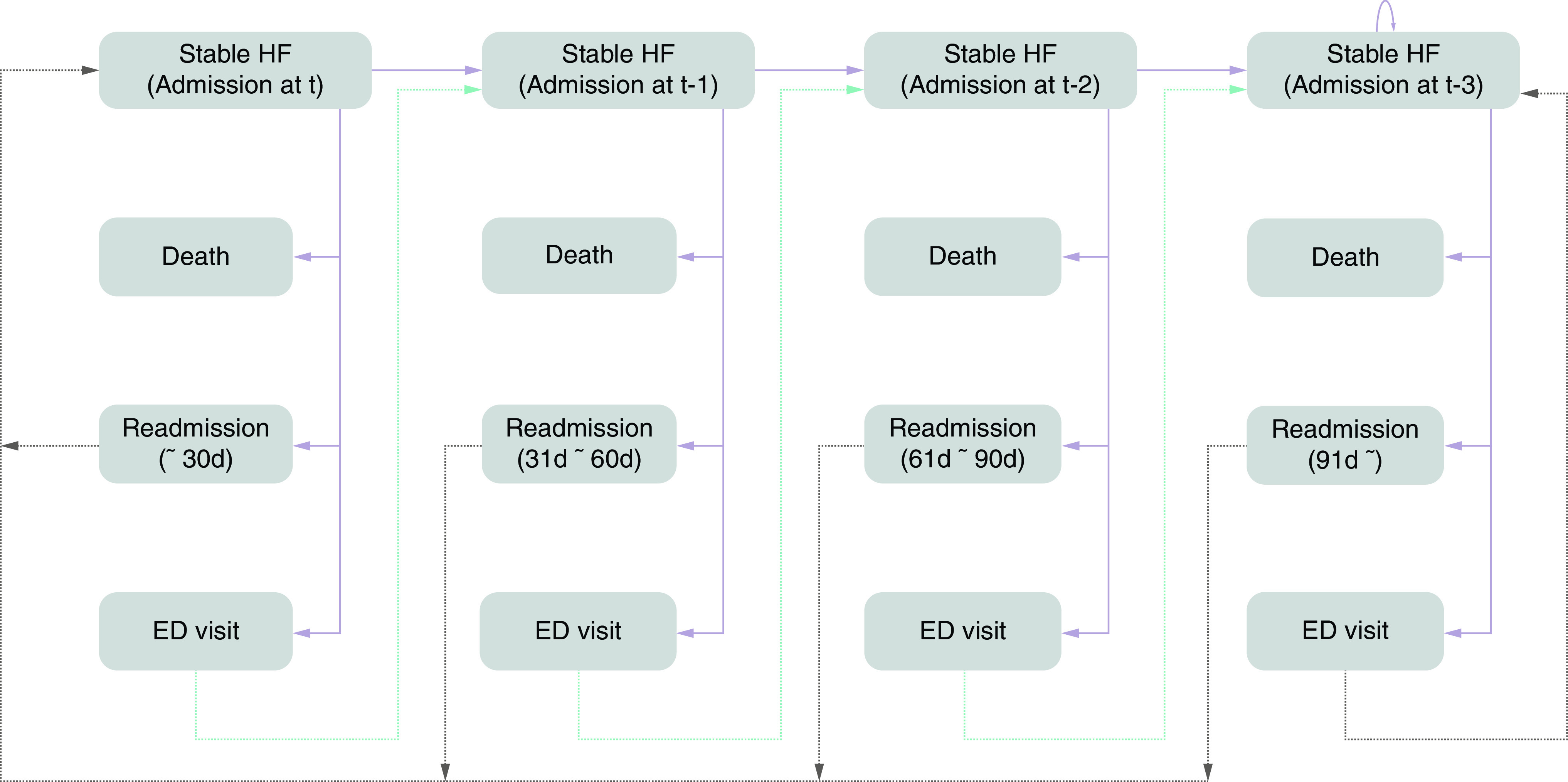
{"title":"索他利氟嗪治疗糖尿病合并近期恶化的心力衰竭患者的成本效益。","authors":"Jaehong Kim, Shanshan Wang, Slaven Sikirica, Jason Shafrin","doi":"10.57264/cer-2023-0190","DOIUrl":null,"url":null,"abstract":"<p><p><b>Aim:</b> To assesses the cost-effectiveness of sotagliflozin for the treatment of patients hospitalized with heart failure and comorbid diabetes. <b>Materials & methods:</b> A <i>de novo</i> cost-effectiveness model with a Markov structure was created for patients hospitalized for heart failure with comorbid diabetes. Outcomes of interest included hospital readmissions, emergency department visits and all-cause mortality measured over a 30-year time horizon. Baseline event frequencies were derived from published real-world data studies; sotagliflozin's efficacy was estimated from SOLOIST-WHF. Health benefits were calculated quality-adjusted life years (QALYs). Costs included pharmaceutical costs, rehospitalization, emergency room visits and adverse events. Economic value was measured using the incremental cost-effectiveness ratio (ICER). <b>Results:</b> Sotagliflozin use decreased annualized rehospitalization rates by 34.5% (0.228 vs 0.348, difference: -0.120), annualized emergency department visits by 40.0% (0.091 vs 0.153, difference: -0.061) and annualized mortality by 18.0% (0.298 vs 0.363, difference: -0.065) relative to standard of care, resulting in a net gain in QAYs of 0.425 for sotagliflozin versus standard of care. Incremental costs using sotagliflozin increased by $19,374 over a 30-year time horizon of the patient, driven largely by increased pharmaceutical cost. Estimated ICER for sotagliflozin relative to standard of care was $45,596 per QALY. <b>Conclusion:</b> Sotagliflozin is a cost-effective addition to standard of care for patients hospitalized with heart failure and comorbid diabetes.</p>","PeriodicalId":15539,"journal":{"name":"Journal of comparative effectiveness research","volume":" ","pages":"e230190"},"PeriodicalIF":2.8000,"publicationDate":"2024-06-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11145521/pdf/","citationCount":"0","resultStr":"{\"title\":\"Cost-effectiveness of sotagliflozin for the treatment of patients with diabetes and recent worsening heart failure.\",\"authors\":\"Jaehong Kim, Shanshan Wang, Slaven Sikirica, Jason Shafrin\",\"doi\":\"10.57264/cer-2023-0190\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p><b>Aim:</b> To assesses the cost-effectiveness of sotagliflozin for the treatment of patients hospitalized with heart failure and comorbid diabetes. <b>Materials & methods:</b> A <i>de novo</i> cost-effectiveness model with a Markov structure was created for patients hospitalized for heart failure with comorbid diabetes. Outcomes of interest included hospital readmissions, emergency department visits and all-cause mortality measured over a 30-year time horizon. Baseline event frequencies were derived from published real-world data studies; sotagliflozin's efficacy was estimated from SOLOIST-WHF. Health benefits were calculated quality-adjusted life years (QALYs). Costs included pharmaceutical costs, rehospitalization, emergency room visits and adverse events. Economic value was measured using the incremental cost-effectiveness ratio (ICER). <b>Results:</b> Sotagliflozin use decreased annualized rehospitalization rates by 34.5% (0.228 vs 0.348, difference: -0.120), annualized emergency department visits by 40.0% (0.091 vs 0.153, difference: -0.061) and annualized mortality by 18.0% (0.298 vs 0.363, difference: -0.065) relative to standard of care, resulting in a net gain in QAYs of 0.425 for sotagliflozin versus standard of care. Incremental costs using sotagliflozin increased by $19,374 over a 30-year time horizon of the patient, driven largely by increased pharmaceutical cost. Estimated ICER for sotagliflozin relative to standard of care was $45,596 per QALY. <b>Conclusion:</b> Sotagliflozin is a cost-effective addition to standard of care for patients hospitalized with heart failure and comorbid diabetes.</p>\",\"PeriodicalId\":15539,\"journal\":{\"name\":\"Journal of comparative effectiveness research\",\"volume\":\" \",\"pages\":\"e230190\"},\"PeriodicalIF\":2.8000,\"publicationDate\":\"2024-06-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11145521/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of comparative effectiveness research\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.57264/cer-2023-0190\",\"RegionNum\":4,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2024/5/21 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q3\",\"JCRName\":\"HEALTH CARE SCIENCES & SERVICES\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of comparative effectiveness research","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.57264/cer-2023-0190","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/5/21 0:00:00","PubModel":"Epub","JCR":"Q3","JCRName":"HEALTH CARE SCIENCES & SERVICES","Score":null,"Total":0}
引用次数: 0
摘要
目的:评估索他利氟嗪治疗心力衰竭合并糖尿病住院患者的成本效益。材料与方法:针对因心力衰竭合并糖尿病而住院的患者,建立一个具有马尔可夫结构的全新成本效益模型。研究结果包括 30 年的再住院率、急诊就诊率和全因死亡率。基线事件频率来自已发表的真实世界数据研究;索他利氟嗪的疗效来自 SOLOIST-WHF 的估算。健康效益按质量调整生命年(QALYs)计算。成本包括药物成本、再住院、急诊就诊和不良事件。经济价值采用增量成本效益比(ICER)进行衡量。研究结果与标准治疗相比,索他利夫罗嗪的年化再住院率降低了34.5%(0.228 vs 0.348,差异:-0.120),年化急诊就诊率降低了40.0%(0.091 vs 0.153,差异:-0.061),年化死亡率降低了18.0%(0.298 vs 0.363,差异:-0.065),因此索他利夫罗嗪与标准治疗相比净收益为0.425 QAYs。在患者 30 年的时间跨度内,使用索他利洛嗪的增量成本增加了 19,374 美元,这主要是由于药物成本增加所致。相对于标准疗法,索他利氟嗪的估计 ICER 为每 QALY 45,596 美元。结论对于因心力衰竭住院并合并糖尿病的患者来说,索他利氟嗪是一种具有成本效益的标准治疗方法。
Cost-effectiveness of sotagliflozin for the treatment of patients with diabetes and recent worsening heart failure.
Aim: To assesses the cost-effectiveness of sotagliflozin for the treatment of patients hospitalized with heart failure and comorbid diabetes. Materials & methods: A de novo cost-effectiveness model with a Markov structure was created for patients hospitalized for heart failure with comorbid diabetes. Outcomes of interest included hospital readmissions, emergency department visits and all-cause mortality measured over a 30-year time horizon. Baseline event frequencies were derived from published real-world data studies; sotagliflozin's efficacy was estimated from SOLOIST-WHF. Health benefits were calculated quality-adjusted life years (QALYs). Costs included pharmaceutical costs, rehospitalization, emergency room visits and adverse events. Economic value was measured using the incremental cost-effectiveness ratio (ICER). Results: Sotagliflozin use decreased annualized rehospitalization rates by 34.5% (0.228 vs 0.348, difference: -0.120), annualized emergency department visits by 40.0% (0.091 vs 0.153, difference: -0.061) and annualized mortality by 18.0% (0.298 vs 0.363, difference: -0.065) relative to standard of care, resulting in a net gain in QAYs of 0.425 for sotagliflozin versus standard of care. Incremental costs using sotagliflozin increased by $19,374 over a 30-year time horizon of the patient, driven largely by increased pharmaceutical cost. Estimated ICER for sotagliflozin relative to standard of care was $45,596 per QALY. Conclusion: Sotagliflozin is a cost-effective addition to standard of care for patients hospitalized with heart failure and comorbid diabetes.
期刊介绍:
Journal of Comparative Effectiveness Research provides a rapid-publication platform for debate, and for the presentation of new findings and research methodologies.
Through rigorous evaluation and comprehensive coverage, the Journal of Comparative Effectiveness Research provides stakeholders (including patients, clinicians, healthcare purchasers, and health policy makers) with the key data and opinions to make informed and specific decisions on clinical practice.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
