Olga Tronina, Michał Brzdęk, Dorota Zarębska-Michaluk, Beata Lorenc, Justyna Janocha-Litwin, Hanna Berak, Marek Sitko, Dorota Dybowska, Włodzimierz Mazur, Magdalena Tudrujek-Zdunek, Ewa Janczewska, Jakub Klapaczyński, Witold Dobracki, Anna Parfieniuk-Kowerda, Rafał Krygier, Łukasz Socha, Robert Flisiak
{"title":"基因型特异性和泛基因型直接作用抗病毒药物对肾功能衰竭的 HCV 感染者的实际疗效。","authors":"Olga Tronina, Michał Brzdęk, Dorota Zarębska-Michaluk, Beata Lorenc, Justyna Janocha-Litwin, Hanna Berak, Marek Sitko, Dorota Dybowska, Włodzimierz Mazur, Magdalena Tudrujek-Zdunek, Ewa Janczewska, Jakub Klapaczyński, Witold Dobracki, Anna Parfieniuk-Kowerda, Rafał Krygier, Łukasz Socha, Robert Flisiak","doi":"10.5114/ceh.2023.133307","DOIUrl":null,"url":null,"abstract":"<p><strong>Aim of the study: </strong>The aim is to summarize the effectiveness and safety of genotype-specific and pangenotypic hepatitis C virus (HCV) treatments in patients with renal failure.</p><p><strong>Material and methods: </strong>In the EpiTer-2 database, which includes data from 22 hepatology centers in Poland, 593 patients with HCV infection and kidney failure were identified. According to KDIGO 2022, they fulfilled the criteria of chronic kidney disease. Patients were divided into two groups: treated with genotype-specific regimens (<i>n</i> = 428) and pangenotypic options (<i>n</i> = 165), in relation to the stage of kidney disease determined using the glomerular filtration rate (GFR) (Cockcroft and Gault equation). Two separate groups were created for hemodialyzed patients (<i>n</i> = 134) and patients after kidney transplantation (<i>n</i> = 89).</p><p><strong>Results: </strong>In a total of 593 patients, 78.7% were treatment-naïve and 23.9% had liver cirrhosis, in 27.5% of cases decompensated. In both groups, the dominant genotype was GT1b. Among patients treated with genotype-specific regimens, LDV/SOF ± RBV, OBV/PTV/r + DSV ± RBV, and GZR/EBR ± RBV treatments were given to 31.5%, 31.5%, and 34.8% of patients respectively. In pangenotypic regimens, GLE/PIB was chosen in 50.3%. Ninety-six percent and 98.8% of patients in the genotype-specific regimen and 88.5% and 94.8% in the pangenotypic regimen achieved a sustained virologic response at 12 weeks (SVR12) in the intention-to-treat and per protocol population respectively. Liver cirrhosis was identified as a risk factor for virological failure. During the study, 14 patients died, 7 in each of the two groups, none related to the antiviral treatment.</p><p><strong>Conclusions: </strong>Both types of treatment regimens are equally effective and safe in patients with renal failure. The stage of renal failure or transplant does not influence the antiviral response.</p>","PeriodicalId":10281,"journal":{"name":"Clinical and Experimental Hepatology","volume":"9 4","pages":"320-334"},"PeriodicalIF":1.7000,"publicationDate":"2023-12-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11103803/pdf/","citationCount":"0","resultStr":"{\"title\":\"Real-world effectiveness of genotype-specific and pangenotypic direct-acting antivirals in HCV-infected patients with renal failure.\",\"authors\":\"Olga Tronina, Michał Brzdęk, Dorota Zarębska-Michaluk, Beata Lorenc, Justyna Janocha-Litwin, Hanna Berak, Marek Sitko, Dorota Dybowska, Włodzimierz Mazur, Magdalena Tudrujek-Zdunek, Ewa Janczewska, Jakub Klapaczyński, Witold Dobracki, Anna Parfieniuk-Kowerda, Rafał Krygier, Łukasz Socha, Robert Flisiak\",\"doi\":\"10.5114/ceh.2023.133307\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Aim of the study: </strong>The aim is to summarize the effectiveness and safety of genotype-specific and pangenotypic hepatitis C virus (HCV) treatments in patients with renal failure.</p><p><strong>Material and methods: </strong>In the EpiTer-2 database, which includes data from 22 hepatology centers in Poland, 593 patients with HCV infection and kidney failure were identified. According to KDIGO 2022, they fulfilled the criteria of chronic kidney disease. Patients were divided into two groups: treated with genotype-specific regimens (<i>n</i> = 428) and pangenotypic options (<i>n</i> = 165), in relation to the stage of kidney disease determined using the glomerular filtration rate (GFR) (Cockcroft and Gault equation). Two separate groups were created for hemodialyzed patients (<i>n</i> = 134) and patients after kidney transplantation (<i>n</i> = 89).</p><p><strong>Results: </strong>In a total of 593 patients, 78.7% were treatment-naïve and 23.9% had liver cirrhosis, in 27.5% of cases decompensated. In both groups, the dominant genotype was GT1b. Among patients treated with genotype-specific regimens, LDV/SOF ± RBV, OBV/PTV/r + DSV ± RBV, and GZR/EBR ± RBV treatments were given to 31.5%, 31.5%, and 34.8% of patients respectively. In pangenotypic regimens, GLE/PIB was chosen in 50.3%. Ninety-six percent and 98.8% of patients in the genotype-specific regimen and 88.5% and 94.8% in the pangenotypic regimen achieved a sustained virologic response at 12 weeks (SVR12) in the intention-to-treat and per protocol population respectively. Liver cirrhosis was identified as a risk factor for virological failure. During the study, 14 patients died, 7 in each of the two groups, none related to the antiviral treatment.</p><p><strong>Conclusions: </strong>Both types of treatment regimens are equally effective and safe in patients with renal failure. The stage of renal failure or transplant does not influence the antiviral response.</p>\",\"PeriodicalId\":10281,\"journal\":{\"name\":\"Clinical and Experimental Hepatology\",\"volume\":\"9 4\",\"pages\":\"320-334\"},\"PeriodicalIF\":1.7000,\"publicationDate\":\"2023-12-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11103803/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Clinical and Experimental Hepatology\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.5114/ceh.2023.133307\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2023/12/15 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q3\",\"JCRName\":\"GASTROENTEROLOGY & HEPATOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Clinical and Experimental Hepatology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.5114/ceh.2023.133307","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2023/12/15 0:00:00","PubModel":"Epub","JCR":"Q3","JCRName":"GASTROENTEROLOGY & HEPATOLOGY","Score":null,"Total":0}
Real-world effectiveness of genotype-specific and pangenotypic direct-acting antivirals in HCV-infected patients with renal failure.
Aim of the study: The aim is to summarize the effectiveness and safety of genotype-specific and pangenotypic hepatitis C virus (HCV) treatments in patients with renal failure.
Material and methods: In the EpiTer-2 database, which includes data from 22 hepatology centers in Poland, 593 patients with HCV infection and kidney failure were identified. According to KDIGO 2022, they fulfilled the criteria of chronic kidney disease. Patients were divided into two groups: treated with genotype-specific regimens (n = 428) and pangenotypic options (n = 165), in relation to the stage of kidney disease determined using the glomerular filtration rate (GFR) (Cockcroft and Gault equation). Two separate groups were created for hemodialyzed patients (n = 134) and patients after kidney transplantation (n = 89).
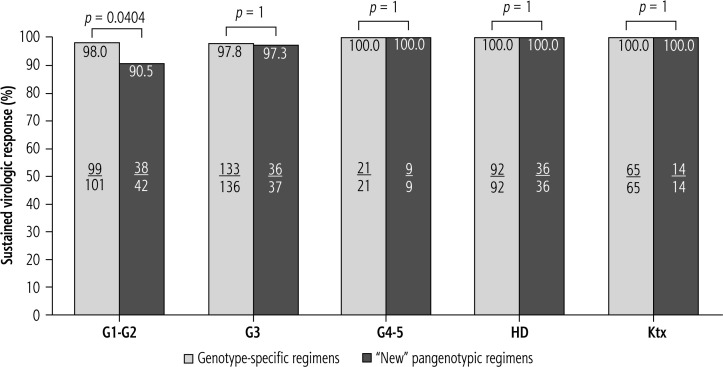
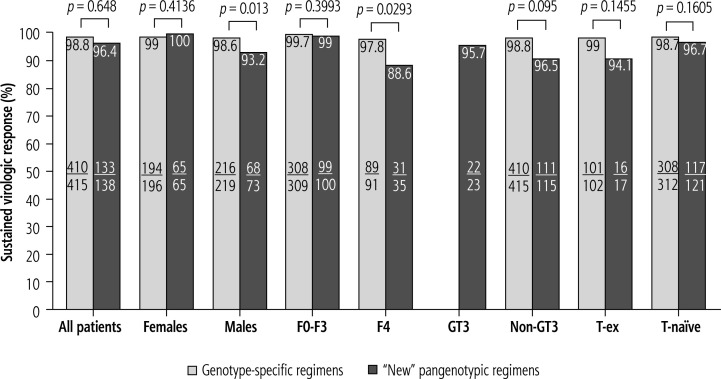
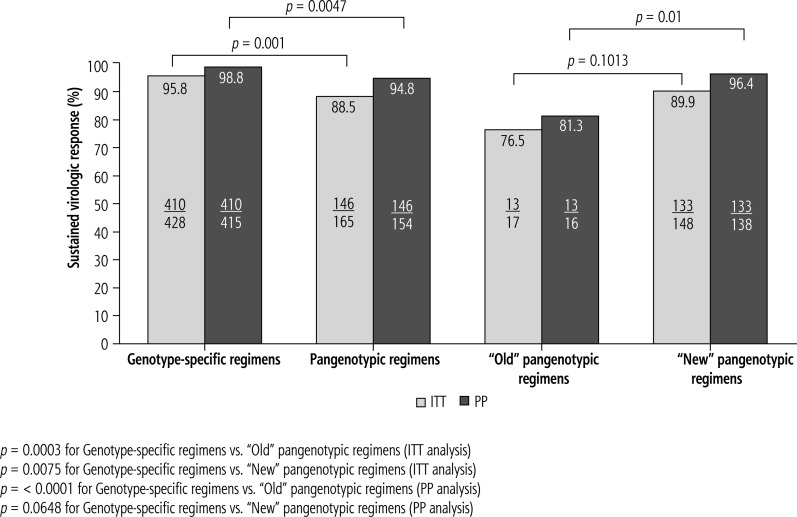
Results: In a total of 593 patients, 78.7% were treatment-naïve and 23.9% had liver cirrhosis, in 27.5% of cases decompensated. In both groups, the dominant genotype was GT1b. Among patients treated with genotype-specific regimens, LDV/SOF ± RBV, OBV/PTV/r + DSV ± RBV, and GZR/EBR ± RBV treatments were given to 31.5%, 31.5%, and 34.8% of patients respectively. In pangenotypic regimens, GLE/PIB was chosen in 50.3%. Ninety-six percent and 98.8% of patients in the genotype-specific regimen and 88.5% and 94.8% in the pangenotypic regimen achieved a sustained virologic response at 12 weeks (SVR12) in the intention-to-treat and per protocol population respectively. Liver cirrhosis was identified as a risk factor for virological failure. During the study, 14 patients died, 7 in each of the two groups, none related to the antiviral treatment.
Conclusions: Both types of treatment regimens are equally effective and safe in patients with renal failure. The stage of renal failure or transplant does not influence the antiviral response.
期刊介绍:
Clinical and Experimental Hepatology – quarterly of the Polish Association for Study of Liver – is a scientific and educational, peer-reviewed journal publishing original and review papers describing clinical and basic investigations in the field of hepatology.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
