Tim Spelman, Sara Eichau, Raed Alroughani, Serkan Ozakbas, Samia J Khoury, Francesco Patti, Eva Kubala Havrdova, Cavit Boz, Murat Terzi, Jens Kuhle, Pierre Grammond, Jeanette Lechner-Scott, Orla Gray, Maria Pia Amato, Guy Laureys, Vahid Shaygannejad, Robert Hyde, Haijue Wang, Ivan Bozin, Nicholas Belviso, Chao Quan, Feng Zeng, Anneke van der Walt, Helmut Butzkueven
{"title":"富马酸二甲酯与非特异性免疫抑制剂的疗效比较:来自 MSBase 的真实世界证据。","authors":"Tim Spelman, Sara Eichau, Raed Alroughani, Serkan Ozakbas, Samia J Khoury, Francesco Patti, Eva Kubala Havrdova, Cavit Boz, Murat Terzi, Jens Kuhle, Pierre Grammond, Jeanette Lechner-Scott, Orla Gray, Maria Pia Amato, Guy Laureys, Vahid Shaygannejad, Robert Hyde, Haijue Wang, Ivan Bozin, Nicholas Belviso, Chao Quan, Feng Zeng, Anneke van der Walt, Helmut Butzkueven","doi":"10.1177/20552173241247182","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>The use of non-specific immunosuppressants (NSIS) to treat multiple sclerosis (MS) remains prevalent in certain geographies despite safety concerns, likely due to resource limitations.</p><p><strong>Objective: </strong>To use MSBase registry data to compare real-world outcomes in adults with relapsing-remitting MS (RRMS) treated with dimethyl fumarate (DMF) or NSIS (azathioprine, cyclosporine, cyclophosphamide, methotrexate, mitoxantrone or mycophenolate mofetil) between January 1, 2014 and April 1, 2022.</p><p><strong>Methods: </strong>Treatment outcomes were compared using inverse probability of treatment weighting (IPTW) Cox regression. Outcomes were annualized relapse rates (ARRs), time to discontinuation, time to first relapse (TTFR) and time to 24-week confirmed disability progression (CDP) or 24-week confirmed disability improvement (CDI; in patients with baseline Expanded Disability Status Scale [EDSS] score ≥2).</p><p><strong>Results: </strong>After IPTW, ARR was similar for DMF (0.13) and NSIS (0.16; <i>p </i>= 0.29). There was no difference in TTFR between cohorts (hazard ratio [HR]: 0.98; <i>p </i>= 0.84). The DMF cohort experienced longer times to discontinuation (HR: 0.75; <i>p </i>= 0.001) and CDP (HR: 0.53; <i>p </i>= 0.001), and shorter time to CDI (HR: 1.99; <i>p </i>< 0.008), versus the NSIS cohort.</p><p><strong>Conclusion: </strong>This analysis supports the use of DMF to treat patients with relapsing forms of MS, and may have implications for MS practices in countries where NSIS are commonly used to treat RRMS.</p>","PeriodicalId":18961,"journal":{"name":"Multiple Sclerosis Journal - Experimental, Translational and Clinical","volume":"10 2","pages":"20552173241247182"},"PeriodicalIF":2.3000,"publicationDate":"2024-05-25","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11128181/pdf/","citationCount":"0","resultStr":"{\"title\":\"Comparative effectiveness of dimethyl fumarate versus non-specific immunosuppressants: Real-world evidence from MSBase.\",\"authors\":\"Tim Spelman, Sara Eichau, Raed Alroughani, Serkan Ozakbas, Samia J Khoury, Francesco Patti, Eva Kubala Havrdova, Cavit Boz, Murat Terzi, Jens Kuhle, Pierre Grammond, Jeanette Lechner-Scott, Orla Gray, Maria Pia Amato, Guy Laureys, Vahid Shaygannejad, Robert Hyde, Haijue Wang, Ivan Bozin, Nicholas Belviso, Chao Quan, Feng Zeng, Anneke van der Walt, Helmut Butzkueven\",\"doi\":\"10.1177/20552173241247182\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>The use of non-specific immunosuppressants (NSIS) to treat multiple sclerosis (MS) remains prevalent in certain geographies despite safety concerns, likely due to resource limitations.</p><p><strong>Objective: </strong>To use MSBase registry data to compare real-world outcomes in adults with relapsing-remitting MS (RRMS) treated with dimethyl fumarate (DMF) or NSIS (azathioprine, cyclosporine, cyclophosphamide, methotrexate, mitoxantrone or mycophenolate mofetil) between January 1, 2014 and April 1, 2022.</p><p><strong>Methods: </strong>Treatment outcomes were compared using inverse probability of treatment weighting (IPTW) Cox regression. Outcomes were annualized relapse rates (ARRs), time to discontinuation, time to first relapse (TTFR) and time to 24-week confirmed disability progression (CDP) or 24-week confirmed disability improvement (CDI; in patients with baseline Expanded Disability Status Scale [EDSS] score ≥2).</p><p><strong>Results: </strong>After IPTW, ARR was similar for DMF (0.13) and NSIS (0.16; <i>p </i>= 0.29). There was no difference in TTFR between cohorts (hazard ratio [HR]: 0.98; <i>p </i>= 0.84). The DMF cohort experienced longer times to discontinuation (HR: 0.75; <i>p </i>= 0.001) and CDP (HR: 0.53; <i>p </i>= 0.001), and shorter time to CDI (HR: 1.99; <i>p </i>< 0.008), versus the NSIS cohort.</p><p><strong>Conclusion: </strong>This analysis supports the use of DMF to treat patients with relapsing forms of MS, and may have implications for MS practices in countries where NSIS are commonly used to treat RRMS.</p>\",\"PeriodicalId\":18961,\"journal\":{\"name\":\"Multiple Sclerosis Journal - Experimental, Translational and Clinical\",\"volume\":\"10 2\",\"pages\":\"20552173241247182\"},\"PeriodicalIF\":2.3000,\"publicationDate\":\"2024-05-25\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11128181/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Multiple Sclerosis Journal - Experimental, Translational and Clinical\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1177/20552173241247182\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2024/4/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q2\",\"JCRName\":\"CLINICAL NEUROLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Multiple Sclerosis Journal - Experimental, Translational and Clinical","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1177/20552173241247182","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/4/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"CLINICAL NEUROLOGY","Score":null,"Total":0}
Comparative effectiveness of dimethyl fumarate versus non-specific immunosuppressants: Real-world evidence from MSBase.
Background: The use of non-specific immunosuppressants (NSIS) to treat multiple sclerosis (MS) remains prevalent in certain geographies despite safety concerns, likely due to resource limitations.
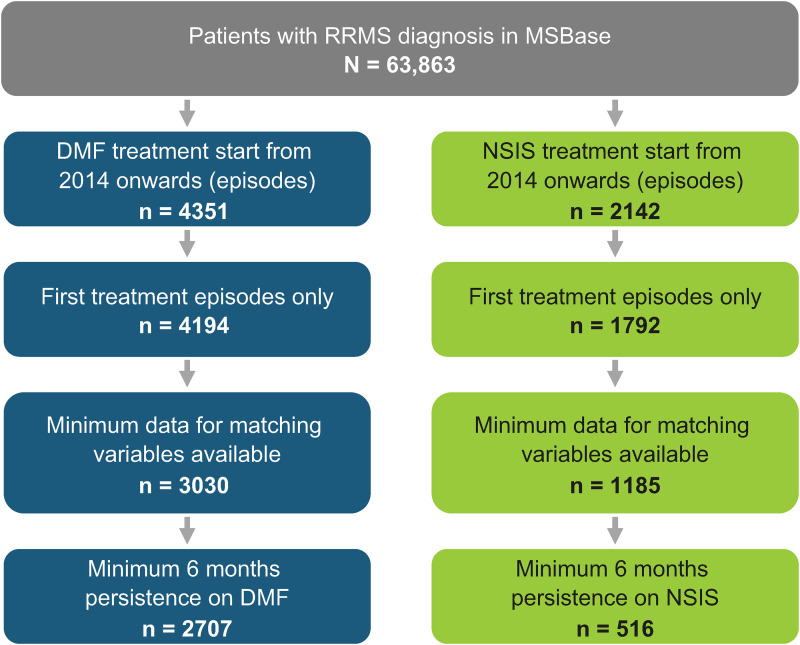
Objective: To use MSBase registry data to compare real-world outcomes in adults with relapsing-remitting MS (RRMS) treated with dimethyl fumarate (DMF) or NSIS (azathioprine, cyclosporine, cyclophosphamide, methotrexate, mitoxantrone or mycophenolate mofetil) between January 1, 2014 and April 1, 2022.
Methods: Treatment outcomes were compared using inverse probability of treatment weighting (IPTW) Cox regression. Outcomes were annualized relapse rates (ARRs), time to discontinuation, time to first relapse (TTFR) and time to 24-week confirmed disability progression (CDP) or 24-week confirmed disability improvement (CDI; in patients with baseline Expanded Disability Status Scale [EDSS] score ≥2).
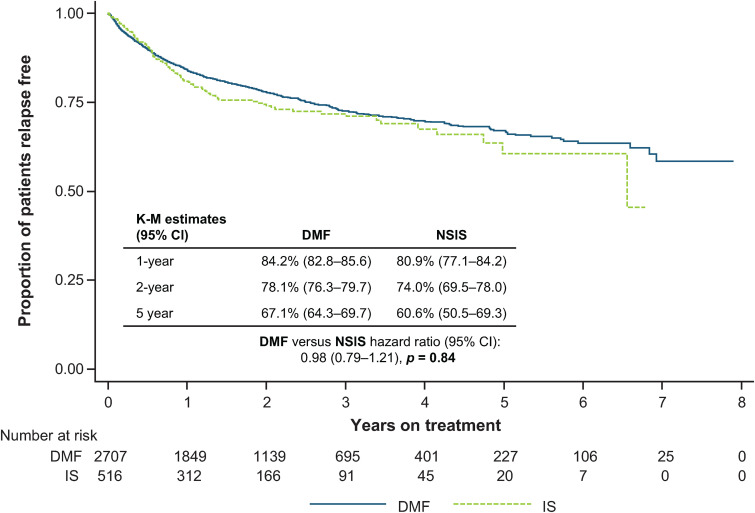
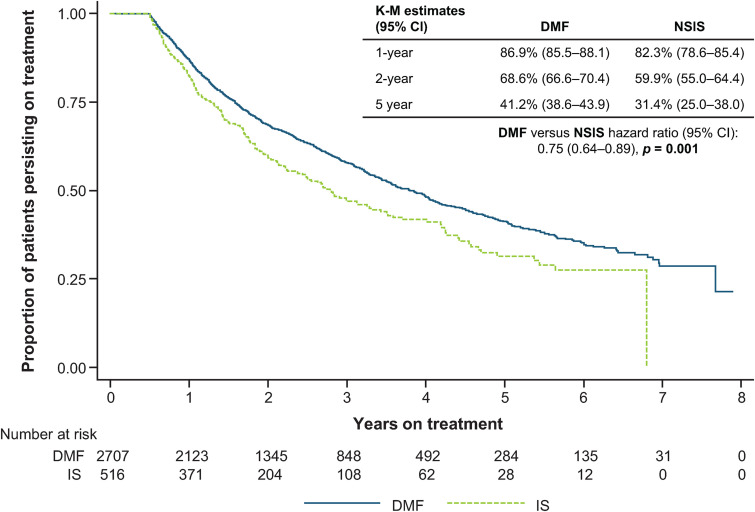
Results: After IPTW, ARR was similar for DMF (0.13) and NSIS (0.16; p = 0.29). There was no difference in TTFR between cohorts (hazard ratio [HR]: 0.98; p = 0.84). The DMF cohort experienced longer times to discontinuation (HR: 0.75; p = 0.001) and CDP (HR: 0.53; p = 0.001), and shorter time to CDI (HR: 1.99; p < 0.008), versus the NSIS cohort.
Conclusion: This analysis supports the use of DMF to treat patients with relapsing forms of MS, and may have implications for MS practices in countries where NSIS are commonly used to treat RRMS.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
