James Y Dai, E Georg Luebeck, Ellen T Chang, Christina A Clarke, Earl A Hubbell, Nan Zhang, Stephen W Duffy
{"title":"在多种癌症类型的随机筛查试验元回归中,晚期癌症的减少与癌症特异性死亡率的降低之间存在密切联系。","authors":"James Y Dai, E Georg Luebeck, Ellen T Chang, Christina A Clarke, Earl A Hubbell, Nan Zhang, Stephen W Duffy","doi":"10.1177/09691413241256744","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Late-stage cancer incidence has been proposed as an early surrogate for mortality in randomized controlled trials (RCTs) of cancer screening; however, its validity has not been systematically evaluated across screening RCTs of different cancers.</p><p><strong>Methods: </strong>We conducted a meta-regression analysis of cancer screening RCTs that reported both late-stage cancer incidence and cancer mortality. Based on a systematic literature review, we included 33 RCTs of screening programs targeting seven cancer types, including lung (<i>n</i> = 12), colorectal (<i>n</i> = 8), breast (<i>n</i> = 5), and prostate (<i>n</i> = 4), among others. We regressed the relative reduction of cancer mortality on the relative reduction of late-stage cancer incidence, inversely weighted for each RCT by the variance of estimated mortality reduction.</p><p><strong>Results: </strong>Across cancer types, the relative reduction of late-stage cancer incidence was linearly associated with the relative reduction of cancer mortality. Specifically, we observed this association for lung (<i>R<sup>2</sup> </i>= 0.79 and 0.996 in three recent large trials), breast (<i>R<sup>2</sup> </i>= 0.94), prostate (<i>R<sup>2</sup> </i>= 0.98), and colorectal cancer (<i>R<sup>2</sup> </i>= 0.75 for stage III/IV cancers and 0.93 for stage IV cancers). Trials with a 20% or greater reduction in late-stage cancers were more likely to achieve a significant reduction in cancer mortality. Our results also showed that no reduction of late-stage cancer incidence was associated with no or minimal reduction in cancer mortality.</p><p><strong>Conclusions: </strong>Meta-regression of historical screening RCTs showed a strong linear association between reductions in late-stage cancer incidence and cancer mortality.</p>","PeriodicalId":51089,"journal":{"name":"Journal of Medical Screening","volume":" ","pages":"211-222"},"PeriodicalIF":2.3000,"publicationDate":"2024-12-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11528850/pdf/","citationCount":"0","resultStr":"{\"title\":\"Strong association between reduction of late-stage cancers and reduction of cancer-specific mortality in meta-regression of randomized screening trials across multiple cancer types.\",\"authors\":\"James Y Dai, E Georg Luebeck, Ellen T Chang, Christina A Clarke, Earl A Hubbell, Nan Zhang, Stephen W Duffy\",\"doi\":\"10.1177/09691413241256744\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Late-stage cancer incidence has been proposed as an early surrogate for mortality in randomized controlled trials (RCTs) of cancer screening; however, its validity has not been systematically evaluated across screening RCTs of different cancers.</p><p><strong>Methods: </strong>We conducted a meta-regression analysis of cancer screening RCTs that reported both late-stage cancer incidence and cancer mortality. Based on a systematic literature review, we included 33 RCTs of screening programs targeting seven cancer types, including lung (<i>n</i> = 12), colorectal (<i>n</i> = 8), breast (<i>n</i> = 5), and prostate (<i>n</i> = 4), among others. We regressed the relative reduction of cancer mortality on the relative reduction of late-stage cancer incidence, inversely weighted for each RCT by the variance of estimated mortality reduction.</p><p><strong>Results: </strong>Across cancer types, the relative reduction of late-stage cancer incidence was linearly associated with the relative reduction of cancer mortality. Specifically, we observed this association for lung (<i>R<sup>2</sup> </i>= 0.79 and 0.996 in three recent large trials), breast (<i>R<sup>2</sup> </i>= 0.94), prostate (<i>R<sup>2</sup> </i>= 0.98), and colorectal cancer (<i>R<sup>2</sup> </i>= 0.75 for stage III/IV cancers and 0.93 for stage IV cancers). Trials with a 20% or greater reduction in late-stage cancers were more likely to achieve a significant reduction in cancer mortality. Our results also showed that no reduction of late-stage cancer incidence was associated with no or minimal reduction in cancer mortality.</p><p><strong>Conclusions: </strong>Meta-regression of historical screening RCTs showed a strong linear association between reductions in late-stage cancer incidence and cancer mortality.</p>\",\"PeriodicalId\":51089,\"journal\":{\"name\":\"Journal of Medical Screening\",\"volume\":\" \",\"pages\":\"211-222\"},\"PeriodicalIF\":2.3000,\"publicationDate\":\"2024-12-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11528850/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of Medical Screening\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1177/09691413241256744\",\"RegionNum\":4,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2024/5/26 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q2\",\"JCRName\":\"PUBLIC, ENVIRONMENTAL & OCCUPATIONAL HEALTH\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Medical Screening","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1177/09691413241256744","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/5/26 0:00:00","PubModel":"Epub","JCR":"Q2","JCRName":"PUBLIC, ENVIRONMENTAL & OCCUPATIONAL HEALTH","Score":null,"Total":0}
Strong association between reduction of late-stage cancers and reduction of cancer-specific mortality in meta-regression of randomized screening trials across multiple cancer types.
Background: Late-stage cancer incidence has been proposed as an early surrogate for mortality in randomized controlled trials (RCTs) of cancer screening; however, its validity has not been systematically evaluated across screening RCTs of different cancers.
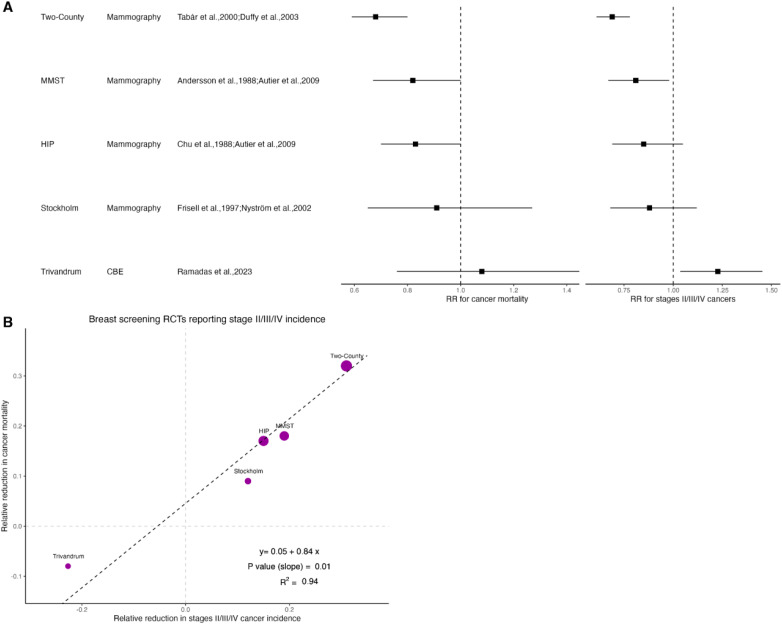
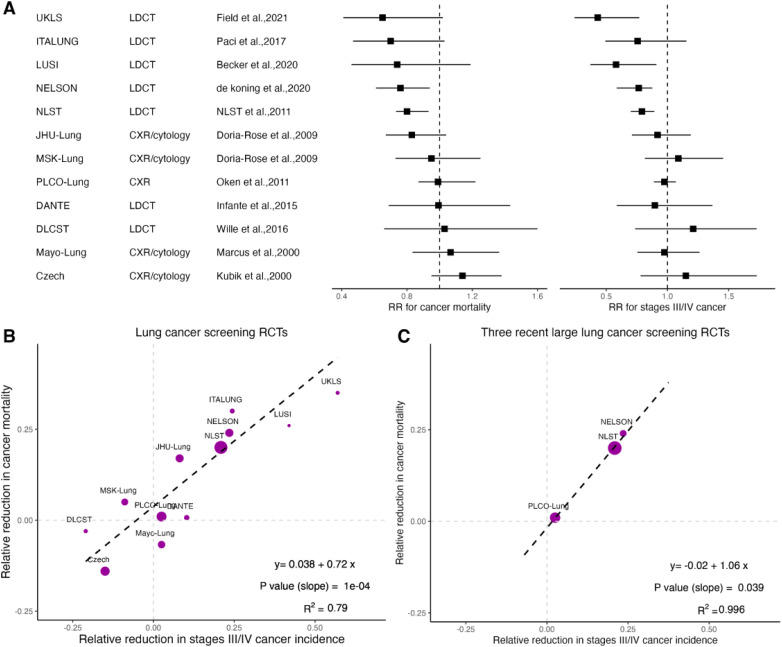
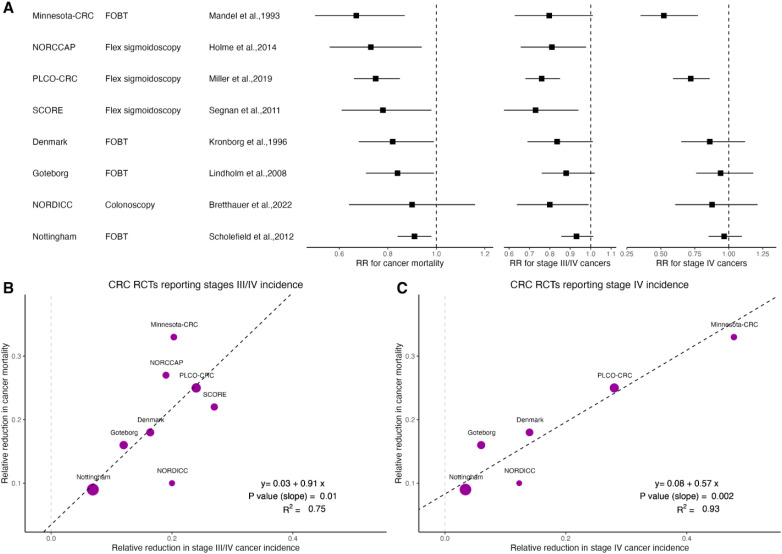
Methods: We conducted a meta-regression analysis of cancer screening RCTs that reported both late-stage cancer incidence and cancer mortality. Based on a systematic literature review, we included 33 RCTs of screening programs targeting seven cancer types, including lung (n = 12), colorectal (n = 8), breast (n = 5), and prostate (n = 4), among others. We regressed the relative reduction of cancer mortality on the relative reduction of late-stage cancer incidence, inversely weighted for each RCT by the variance of estimated mortality reduction.
Results: Across cancer types, the relative reduction of late-stage cancer incidence was linearly associated with the relative reduction of cancer mortality. Specifically, we observed this association for lung (R2= 0.79 and 0.996 in three recent large trials), breast (R2= 0.94), prostate (R2= 0.98), and colorectal cancer (R2= 0.75 for stage III/IV cancers and 0.93 for stage IV cancers). Trials with a 20% or greater reduction in late-stage cancers were more likely to achieve a significant reduction in cancer mortality. Our results also showed that no reduction of late-stage cancer incidence was associated with no or minimal reduction in cancer mortality.
Conclusions: Meta-regression of historical screening RCTs showed a strong linear association between reductions in late-stage cancer incidence and cancer mortality.
期刊介绍:
Journal of Medical Screening, a fully peer reviewed journal, is concerned with all aspects of medical screening, particularly the publication of research that advances screening theory and practice. The journal aims to increase awareness of the principles of screening (quantitative and statistical aspects), screening techniques and procedures and methodologies from all specialties. An essential subscription for physicians, clinicians and academics with an interest in screening, epidemiology and public health.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
