Nidharshan Subra Anandasivam, Jaya Vasudevan, Holli Sadler, Christopher Moriates, Michael Pignone
{"title":"由住院医师主导的改进项目,在门诊中筛查抵抗性高血压患者的原发性高醛固酮血症。","authors":"Nidharshan Subra Anandasivam, Jaya Vasudevan, Holli Sadler, Christopher Moriates, Michael Pignone","doi":"10.1136/bmjoq-2023-002611","DOIUrl":null,"url":null,"abstract":"<p><p>Clinical practice guidelines recommend screening for primary hyperaldosteronism (PH) in patients with resistant hypertension. However, screening rates are low in the outpatient setting. We sought to increase screening rates for PH in patients with resistant hypertension in our Veterans Affairs (VA) outpatient resident physician clinic, with the goal of improving blood pressure control. Patients with possible resistant hypertension were identified through a VA Primary Care Almanac Metric query, with subsequent chart review for resistant hypertension criteria. Three sequential patient-directed cycles were implemented using rapid cycle improvement methodology during a weekly dedicated resident quality improvement half-day. In the first cycle, patients with resistant hypertension had preclinic PH screening labs ordered and were scheduled in the clinic for hypertension follow-up. In the second cycle, patients without screening labs completed were called to confirm medication adherence and counselled to screen for PH. In the third cycle, patients with positive screening labs were called to discuss mineralocorticoid receptor antagonist (MRA) initiation and possible endocrinology referral. Of 97 patients initially identified, 58 (60%) were found to have resistant hypertension while 39 had pseudoresistant hypertension from medication non-adherence. Of the 58 with resistant hypertension, 44 had not previously been screened for PH while 14 (24%) had already been screened or were already taking an MRA. Our screening rate for PH in resistant hypertension patients increased from 24% at the start of the project to 84% (37/44) after two cycles. Of the 37 tested, 24% (9/37) screened positive for PH, and 5 patients were started on MRAs. This resident-led quality improvement project demonstrated that a focused intervention process can improve PH identification and treatment.</p>","PeriodicalId":9052,"journal":{"name":"BMJ Open Quality","volume":"13 2","pages":""},"PeriodicalIF":1.6000,"publicationDate":"2024-05-27","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11131109/pdf/","citationCount":"0","resultStr":"{\"title\":\"Resident-led improvement project to screen for primary hyperaldosteronism in patients with resistant hypertension in an outpatient clinic.\",\"authors\":\"Nidharshan Subra Anandasivam, Jaya Vasudevan, Holli Sadler, Christopher Moriates, Michael Pignone\",\"doi\":\"10.1136/bmjoq-2023-002611\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>Clinical practice guidelines recommend screening for primary hyperaldosteronism (PH) in patients with resistant hypertension. However, screening rates are low in the outpatient setting. We sought to increase screening rates for PH in patients with resistant hypertension in our Veterans Affairs (VA) outpatient resident physician clinic, with the goal of improving blood pressure control. Patients with possible resistant hypertension were identified through a VA Primary Care Almanac Metric query, with subsequent chart review for resistant hypertension criteria. Three sequential patient-directed cycles were implemented using rapid cycle improvement methodology during a weekly dedicated resident quality improvement half-day. In the first cycle, patients with resistant hypertension had preclinic PH screening labs ordered and were scheduled in the clinic for hypertension follow-up. In the second cycle, patients without screening labs completed were called to confirm medication adherence and counselled to screen for PH. In the third cycle, patients with positive screening labs were called to discuss mineralocorticoid receptor antagonist (MRA) initiation and possible endocrinology referral. Of 97 patients initially identified, 58 (60%) were found to have resistant hypertension while 39 had pseudoresistant hypertension from medication non-adherence. Of the 58 with resistant hypertension, 44 had not previously been screened for PH while 14 (24%) had already been screened or were already taking an MRA. Our screening rate for PH in resistant hypertension patients increased from 24% at the start of the project to 84% (37/44) after two cycles. Of the 37 tested, 24% (9/37) screened positive for PH, and 5 patients were started on MRAs. This resident-led quality improvement project demonstrated that a focused intervention process can improve PH identification and treatment.</p>\",\"PeriodicalId\":9052,\"journal\":{\"name\":\"BMJ Open Quality\",\"volume\":\"13 2\",\"pages\":\"\"},\"PeriodicalIF\":1.6000,\"publicationDate\":\"2024-05-27\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11131109/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"BMJ Open Quality\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1136/bmjoq-2023-002611\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q4\",\"JCRName\":\"HEALTH CARE SCIENCES & SERVICES\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"BMJ Open Quality","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1136/bmjoq-2023-002611","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q4","JCRName":"HEALTH CARE SCIENCES & SERVICES","Score":null,"Total":0}
Resident-led improvement project to screen for primary hyperaldosteronism in patients with resistant hypertension in an outpatient clinic.
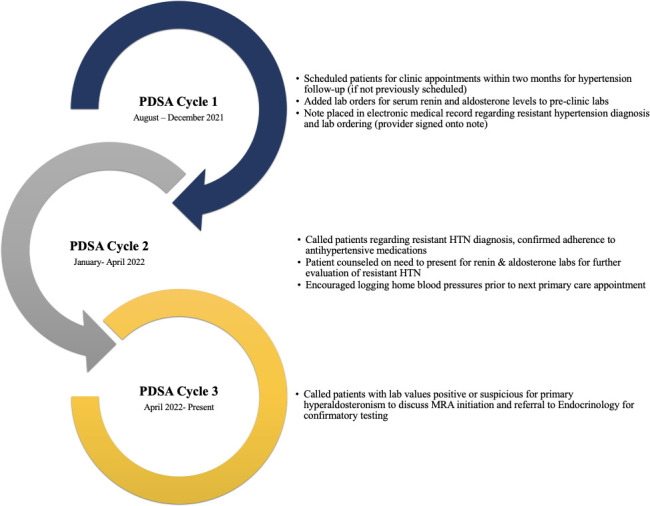
Clinical practice guidelines recommend screening for primary hyperaldosteronism (PH) in patients with resistant hypertension. However, screening rates are low in the outpatient setting. We sought to increase screening rates for PH in patients with resistant hypertension in our Veterans Affairs (VA) outpatient resident physician clinic, with the goal of improving blood pressure control. Patients with possible resistant hypertension were identified through a VA Primary Care Almanac Metric query, with subsequent chart review for resistant hypertension criteria. Three sequential patient-directed cycles were implemented using rapid cycle improvement methodology during a weekly dedicated resident quality improvement half-day. In the first cycle, patients with resistant hypertension had preclinic PH screening labs ordered and were scheduled in the clinic for hypertension follow-up. In the second cycle, patients without screening labs completed were called to confirm medication adherence and counselled to screen for PH. In the third cycle, patients with positive screening labs were called to discuss mineralocorticoid receptor antagonist (MRA) initiation and possible endocrinology referral. Of 97 patients initially identified, 58 (60%) were found to have resistant hypertension while 39 had pseudoresistant hypertension from medication non-adherence. Of the 58 with resistant hypertension, 44 had not previously been screened for PH while 14 (24%) had already been screened or were already taking an MRA. Our screening rate for PH in resistant hypertension patients increased from 24% at the start of the project to 84% (37/44) after two cycles. Of the 37 tested, 24% (9/37) screened positive for PH, and 5 patients were started on MRAs. This resident-led quality improvement project demonstrated that a focused intervention process can improve PH identification and treatment.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
